

Can we eradicate maladministration of expressed breast milk using a risk analysis approach?
Reported errors of expressed breast milk (EBM) administration (specifically, feeding a mother’s EBM to the wrong infant) were analysed for a tertiary neonatal intensive and special care unit. Interventions aimed at reducing errors during a seven-year period were reviewed. As a result, we propose a potential solution to further improve the process of EBM administration. We hope that by highlighting our project to the wider neonatal community, we might promote discussion around the handling of EBM and potential maladministration.
Charlotte A. CardMBBS, MRCPCH
Paediatric ST4 trainee
c.card@nhs.net Katy Barnes
MBBS, MRCPCH
Neonatal Registrar Philip Amess
MBBS, MRCP
Consultant Neonatologist
Department of Neonatology, Trevor Mann Baby Unit, Royal Sussex County Hospital
Background
Breast milk is recommended as the optimal source of nutrition for newborn infants. This is especially the case for preterm infants where there is evidence for improving feed tolerance, immunological function, neurodevelopmental outcomes and reducing the rate of necrotising enterocolitis.1 For a large proportion of the preterm and very sick infants in a neonatal unit, most enteral nutrition will be administered as expressed breast milk (EBM) via a gastric tube. Much effort is made to support mothers with expressing breast milk and ensuring that it is safely administered and stored.
As a tertiary neonatal unit with approximately 550 admissions per year, we estimate that approximately 38,000 EBM feeds are given annually. The vast majority of these feeds will be given uneventfully but this is not always the case. Errors in breast milk administration are fortunately rare but it is important to ensure consis-tent delivery of the correct mother’s EBM to her baby (TABLE 1). This can be a challenge when administering so many feeds; nevertheless, errors are a failure of optimal care and cause a great deal of stress for all involved, potentially leading to a breakdown in trust between staff and parents.
We and others have developed guidelines for the safe handling of breast milk2 but in reality, we recognise the difficulty in eradicating all errors related to providing what should be a completely positive and risk-free source of nutrition for our babies. We therefore decided to review our breast milk administration errors and near-miss events, and our interventions aimed at reducing such errors with a view to undertaking a quality improvement (QI) project. These errors have been formally reported using our trust’s incident reporting system, Datix.
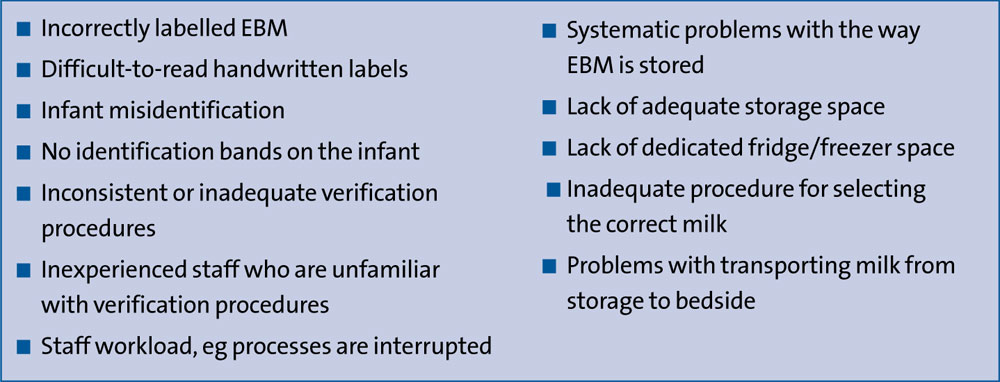
TABLE 1 Factors that might contribute to an infant receiving the wrong mother’s EBM.
Methodology
We looked at breast milk administration during a seven-year period (2012-2018) at the Brighton and Sussex University Hospitals NHS Trust including the Trevor Mann Baby Unit (TMBU) at Royal Sussex County Hospital and the eight-bedded special care baby unit (SCBU) at Princess Royal Hospital. TMBU is a regional neonatal surgical intensive care unit with 27 cots and approximately 550 admissions (8,800 cot days) annually. All staff within the trust are encouraged to report clinical incidents using the Datix reporting system. The Datix reports relating to breast milk administration between 2012 and 2018 were retrieved and each case was reviewed to analyse the type of error involved and the interventions undertaken to determine their effectiveness in improving the administration process.
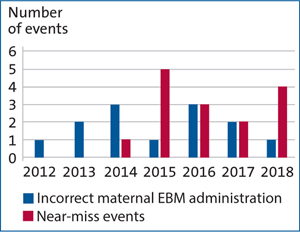
FIGURE 1 Reported clinical incidents relating to EBM administration, 2012 to 2018.
Analysis of incident reports
Between 2012 and 2018, a total of 33 clinical incidents were reported relating to errors in enteral milk administration. Five cases were excluded from analysis as the cases reported related to formula milk or incorrect frequency of feeding.
Therefore, a total of 28 clinical incidents relating to EBM maladministration were identified (FIGURE 1). These included:
- 13 cases of incorrect EBM administration, ie the infant received the wrong mother’s EBM
- 15 ‘near miss’ events, ie a potential error was recognised early enough to avoid incorrect administration.
From the incident description in the reports, the errors could be grouped into different categories (FIGURE 2) including incorrect labelling, storage and checking procedures.
Although several types of errors were seen to contribute to the incorrect administration of EBM, one of the most common types of error was the failure of the pre-administration checking procedure (29%). In eight cases, failure of the pre-administration checking procedure inevitably led to the wrong EBM being given to the baby.
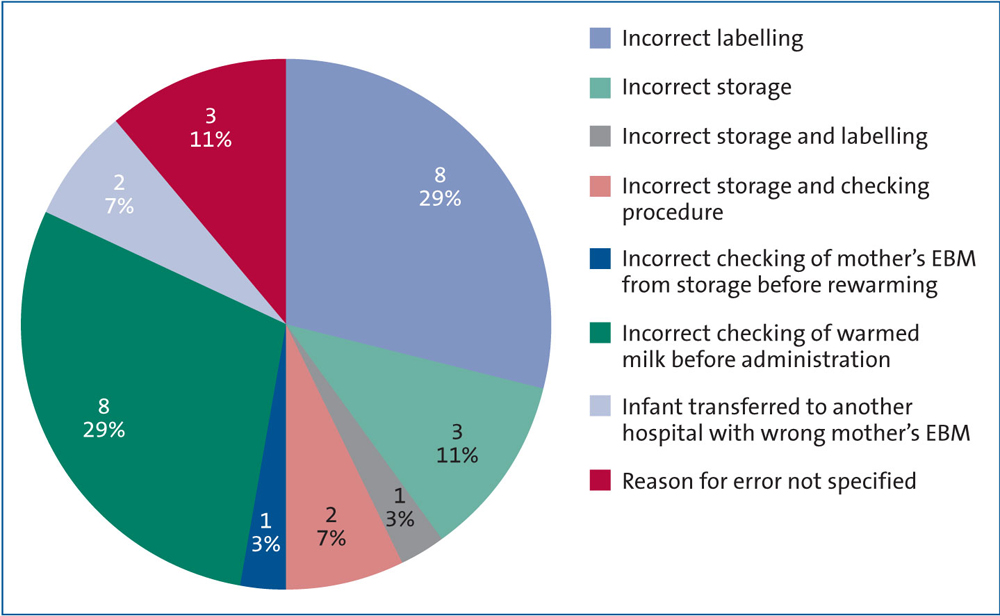
FIGURE 2 A pie chart to illustrate the types of errors leading to the reported incidents.
Analysis of interventions
Commonly, medical errors are a result of imperfect processes, adverse conditions leading to human mistakes, or failure of prevention strategies.3There are a number of potential stages during the feeding process that could lead to error including collection, storage, preparation and administration of breast milk. This is compounded by the number of individuals involved in the process, the high number of feeds given each day on the unit and environmental factors including excessive workload, availability of feed warmers and staff shortages. Unlike some neonatal units, only three feed warmers are available in each nursery (due to lack of space) rather than one for each cot space.
Between 2012 and 2018, several interventions have been undertaken to reduce our errors in breast milk administration:
- Labelling EBM at the bedside with full patient demographics
- An education programme for staff
- Printed labels for EBM with patient demographics
- Special alerts in the ‘Baby Watch’ department safety bulletin
- Two-person check introduced at the cot side against patient wristband
- Second check introduced immediately prior to administration by two nurses
During 2015, single nurse checking procedures were implemented including checks when the milk is drawn up for warming, prior to administration and against the nasogastric tube label during the feed. This was changed to include two nurses at each checking stage during 2017-2018.
The current process for milk administration is shown in FIGURE 3.
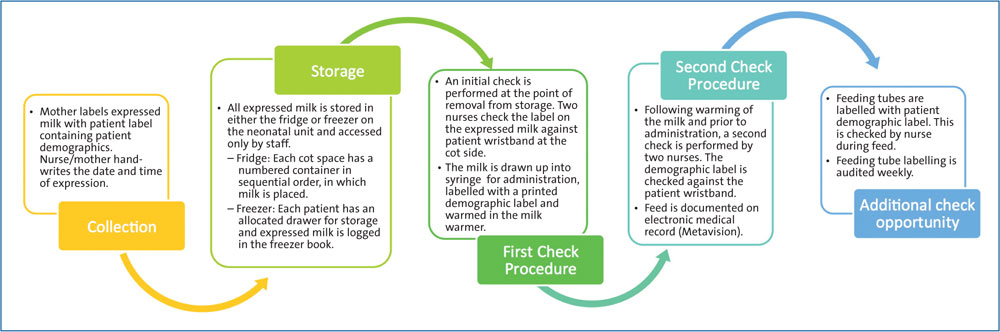
FIGURE 3 The current process for EBM handling and administration at TMBU.
Conclusion of investigation
Although the number of incidents is small in comparison to the number of feeds given, the impact is disproportionately high. The significant negative impact of such errors includes:
- risk of transmission of infection4 as breast milk is classified as a bodily fluid similar to blood or plasma
- in-depth and time-consuming investigation of potential infection
- financial impact of additionalinvestigations
- emotional and psychological impacton parents
- loss of confidence and mistrust in the care received on the neonatal unit by the families involved
- the risk that a mother may decide not to feed her baby breast milk because of a fear of maladministration.
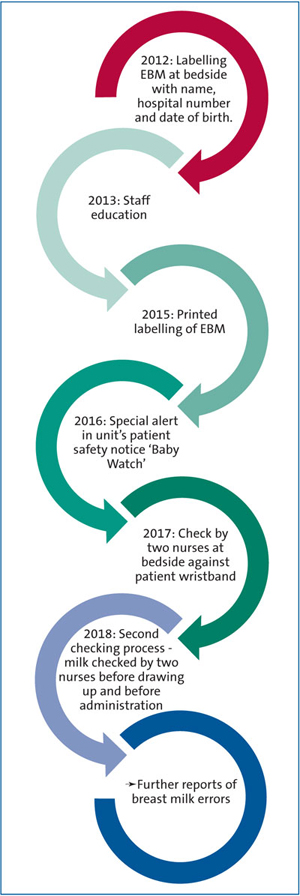
FIGURE 4 Interventions to improve the process of breast milk administration during the period 2012-2018.
Despite numerous interventions to educate and improve the feeding process (FIGURE 4), we continued to see incidents. As shown in FIGURE 1, from 2016-18 there was a reduction in the number of incorrect EBM administration events and an increase in reported near-miss events. This could suggest changes to checking procedures during this period had some benefit, however ultimately errors were not completely eradicated.
Clinical incident reporting is useful in the detection of errors within clinical processes, however system changes as a result of these reports are not effective enough in preventing incidents, as similarly described by Zeilhofer et al.5 We postulate this is a result of the difficulty to completely exclude the impact of human error on medical processes. Although interventions can have a positive impact in the short-term, the desired effect is often unsustained.6
Proposed solution for QI initiative
It is important to identify the risk factors that may lead to an infant receiving incorrect EBM and implement strategies to mitigate the risk of EBM maladministra-tion. In order to prevent mistakes, it is necessary to create medical systems that ‘make it hard for people to do the wrong thing and easy for people to do the right thing’.3 The introduction of a medical barcode tracking system specifically for the administration of EBM on the unit would aim to further remove human factors leading to the wrong administration of milk. This system is already used on our unit for labelling of EBM, for bedside phlebotomy and for the administration of blood products. The Bloodhound system (MSoft eSolutions Ltd) consists of a barcoded identification wristband for each patient and a handheld portable computer that can scan the barcode to confirm positive identification and print patient-specific labels.
There is significant evidence in the literature that barcoded electronic identification systems improve patient safety during blood transfusions and medication administration.7-8 We aim to adapt our current tracking system further to allow for barcode matching between infants and their EBM to ensure safe administration. Similar initiatives are reported to have had significant benefits in preventing human milk errors on neonatal intensive care units in the United States and Canada.9-10 This change will be implemented on our unit between 2019 and 2020. We will be following a plan-do-study-act (PDSA) cycle quality improvement method to implement and review our proposed solution (FIGURE 5).
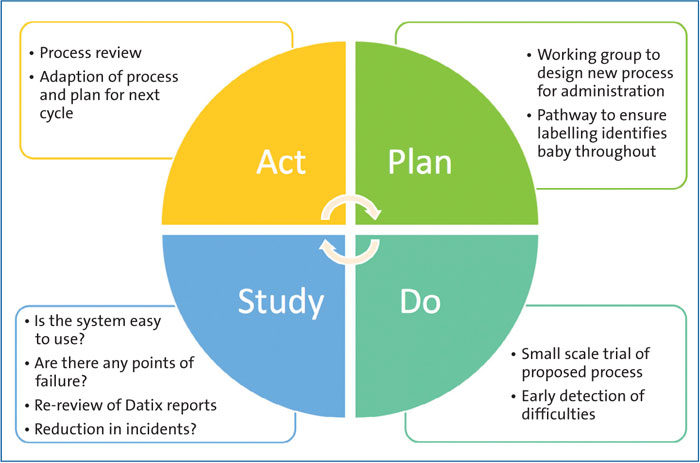
FIGURE 5 PDSA cycle for service improvement.
Through our discussions with other units, in and out of our local operational delivery network, we believe that breast milk administration errors will also be occurring with similar frequency else-where. As guidelines for prevention of error are not universal across other neonatal units, it is likely that such events are under-reported. We hope that by sharing our experiences, we can promote discussion and QI initiatives.
Or read this article in our
Tablet/iPad edition
- Despite rates of breast milk maladministration being relatively low there are potentially serious implications when the wrong mother’s breast milk is given to an infant.
- QI interventions, such as staff education and additional safety checks, may not have the desired or sustained effects.
- Complete elimination of human errors during a medical process is likely to pose a significant challenge. However, medical barcode tracking systems specifically for EBM may help to prevent maladministration.
Also published in Infant:
