

Video vs direct laryngoscopy. Success rates and confidence: a feasibility study
Video-assisted laryngoscopy (VL) is being used increasingly in adult, paediatric and neonatal populations although its use has not been extensively studied in a neonatal setting. The authors’ experiences on the neonatal unit suggested that there is increased team confidence around tube or catheter placement and intubation is more successful when trainee and trainer are able to view the procedure using a video screen. This article outlines a study that looks at this theory.
David G. Bartle1
MBChB, MRCPCH
Consultant Paediatrician, Trust Simulation Lead, Neonatal Clinical Lead
david.bartle@nhs.net
Roy Powell2,3
BSc(Hons), PhD, CBIOL, FSB, FHEA
Research Design Consultant
Katie Pearson1
MBChB, MRCPCH
Paediatric Registrar
Teniola S. Adeboye3
Medical Student
2Royal Devon and Exeter NHS Foundation Trust
3University of Exeter Medical School
Background
Neonatal intubation can be technically difficult and success rates for real-time neonatal intubation suboptimal.1 It is a core skill for paediatric trainees. Opportunities for trainees to perform neonatal intubation are decreasing due to less invasive methods of ventilator support, fewer intubations being performed on neonatal units, centralisation of specialist services and less hours worked by trainees due to the enforcement of the European Working Time Directive. Increasingly the less invasive surfactant administration (LISA) technique is being used. With the use of catheter insertion, it is impossible to use an end tidal carbon dioxide monitor to check placement. VL can improve team confidence around this placement prior to surfactant administration.
What is already known?
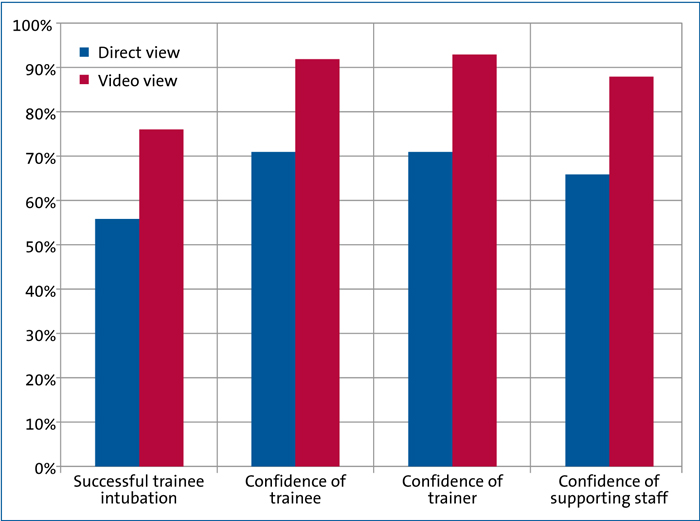
Intubation success rates of inexperienced neonatal trainees significantly improved when the instructor was able to share their view on a video laryngoscope screen.2 In adults, VL is used routinely in a lot of hospitals. It has been shown that education using a video system improves intubation skills in medical students for adult intubation.3 VL is also being used increasingly in paediatric intensive care units and in paediatric emergency departments. VL is associated with greater first time success in the paediatric emergency department setting.4 With traditional direct laryngoscopy (DL), a viewing angle of approximately 15 degrees is achieved. With the video laryngoscope this is up to 85 degrees as the camera is at the distal end of the blade along with the bulb. The Storz C-Mac video laryngoscope is a similar shape and size to a conventional laryngoscope, therefore technique for intubation is the same. The handle is slightly broader (FIGURE 1). FIGURE 1 Storz C-Mac blades old (above) and new (below) showing the difference in the blade tip. In neonatal resuscitation there is approximately a 62% success rate on each attempt for intubation with DL ranging from 24% (residents) to 86% (consultants).1 A previous study showed the success rate of intubation on a neonatal manikin is improved and oesophageal intubation decreased while learning intubation using VL compared to DL. Although time to successful intubation is longer using VL, the time difference is not clinically significant. Once intubation is mastered on manikins using VL, this competence is easily transferred to the use of DL.5 When the supervisor shares the view that the trainee has, by viewing on a video screen, trainee success rates are increased.6 In a simulation environment there was no improvement in performance when using video vs direct view7 and there was no difference in number of attempts or time to achieve intubation when comparing VL vs DL in a 2018 Cochrane review.8 Having used a Storz C-Mac video laryngoscope extensively, the authors felt that the success rate for intubation of our paediatric trainees and team confidence around tube and catheter placement was significantly improved by the use of the video laryngoscope. One concern was that the trainee who has learnt intubation using VL may find it difficult to perform intubation by DL. However, medical students who learnt intubation using the video were no less likely to succeed and in fact there was a tendency to improved successful intubation.2 The aim of this study was to determine the feasibility of comparing intubation of newborn babies by VL with laryngoscopy by direct view. The aims of a future main study would be to measure whether there are fewer attempts at intubation using the video and whether team confidence concerning endotracheal tube (ETT) placement is improved when the whole team can view the procedure. A feasibility study was designed in which patients were randomised to VL or DL for intubation on a neonatal unit between August 2016 and March 2018. The target was to recruit 40 babies in order to provide sufficient data to determine standard deviations of continuous measures. The study was run across two sites: Oral intubation was performed and any infant who required intubation was eligible for inclusion in the study. Infants were not recruited if they were in extremis requiring immediate intubation by a senior exper-ienced operator who used his/her own preferred method. Infants who were to be intubated nasally were not included as this technique is not usually taught to registrars. Any baby with a congenital airway malformation was not included in the study. None of the procedures were emergency delivery room intubations. Some babies were excluded as they were felt to be too small for the equipment to be effective (the distance between light source and blade tip was too small so visualisation was impossible). Attempts to successful intubation were recorded as was confidence of the trainer, trainee and nursing staff in success of intubation. Successful intubation was determined by the doctors being satisfied that the ETT was in the trachea and the baby was being ventilated. This was initially determined clinically, but subsequently confirmed by a chest radiograph with or without capnography. An unsuccessful intubation was defined as the ETT being placed and removed, or the attempt at intubation stopped, the baby re-oxygenated and a further attempt made. Trainees were allowed no more than three attempts at intubation in either arm of the study. For both groups, direction was given to the trainee during the attempt at intubation. Advice included depth of insertion of the laryngoscope blade and amount of elevation of the blade needed. For the VL group, further direction was given once the vocal cords were seen; however, this could not be replicated without video as a shared view was not available. In the case of the direct view, the assessor was able to look down the laryngoscope blade to look for the cords if needed and direction given. A Storz C-Mac video laryngoscope was used with a size 1 or size 0 Millar blade for the video view and a standard neonatal laryngoscope was used for direct view. Intubations were performed by a junior doctor (F2 or ST trainee) and supervised by a senior doctor (consultant or senior trainee). Ethics approval was sought in order to proceed with the study. Consent was initially prospective, however during the study, ethics approval was granted for randomisation to VL or DV and retro-spective request made to the parents to use the details around the time of intubation. The request was not for the use of VL as this is considered standard equipment on a neonatal unit. Consent was also sought from the trainee as details of their attempts were recorded. Both parents and trainee were given a study information leaflet. Randomisation was performed using concealment of allocation; a statistician (RP) provided a block randomisation list. This ensured that the envelopes were distributed evenly between the two units. The number of attempts to success of intubation was recorded fot this study. ETT position was checked, as is routinely performed after any intubation. Confidence of accurate tube placement at the time of intubation was recorded using a five-point rating scale by the staff involved in the intubation, including trainee, trainer and other supporting staff (usually an assisting nurse). The rating scale was scored individually and separately by trainee, trainer and nurse assisting with the intubation. The score was based on the confidence of the healthcare professionals that the ETT had been successfully placed at the time of tube placement. Number of attempts at intubation isn’t routinely collected, however there was a data sheet to collect this information. The research and development team performed independent data collection and entry of the data to remove potential bias. A sample size of 40 babies was deemed necessary to look at feasibility of conduct-ing the main trial, ie 20 babies in each arm. In terms of throughput, 150 babies have been intubated in Exeter over the last three years, with approximately 200-250 intubations per year at Derriford Hospital. Descriptive analyses were conducted giving means and standard deviations of outcome scores or median and inter-quartile ranges (IQR) where appropriate if the data were not normally distributed and could not be easily transformed. This applied to the various visual analogue scale scores. Estimates of central tendency and variation enabled a sample size calculation to be conducted in order to power a larger definitive trial at a later date. The statistician analysing the data was blinded to group allocation. Forty intubations were performed across both sites (26 in Exeter and 14 in Plymouth). Twenty-one babies were allocated to the VL group and 18 to DL with one patient that was allocated to the direct view group withdrawn. Despite rigorous randomisation, the babies in the VL group were heavier: mean 2.62kg vs 2.04kg, but this was not significant (p=0.06). The median age at intubation was the same in each group with differing IQR reflecting a larger range of age in the DL group: 1 (IQR=2) days (VL) vs 1 (IQR=17) days (DL). Two thirds of babies hadn’t been intubated before; one third had and these were older with a median of 32 (IQR=92) days, compared with 1 day (IQR=1) for those that had not. All babies received paralysis (suxemeth-onium or vecuronium). There was similar experience of previous intubations by trainees between the two groups. However, the VL group had six trainees who had not intubated before vs one in the DL group. 76% (16/21, 95% CI: 53% to 92%) of trainees who used VL were successful at intubation vs 56% (10/18, 95% CI: 31% to 78%) using DL (FIGURE 2). The number of attempts to successful intubation was fewer in the VL group median 1.5 (IQR=1.5) vs the DL group median 2 (IQR=1). FIGURE 2 Success rates and confidence of trainees and staff. Confidence of tube placement was also increased among the VL group with median trainee confidence at 99% (IQR=6%); vs 86.5% (IQR=43%) in the DL group. Trainer median confidence was 94% (IQR=10%) in the VL group vs 86% (IQR=19%) in the DL group. The median confidence of supporting staff was 88.5% (IQR=11%) in the VL group vs 74% (IQR=35%) in the DL group. As this was feasibility work, testing for significance was not appropriate. The emphasis was more about whether a study of this nature can be performed with neonates and VL. The sample size for a future definitive trial based on 76% success in intubation in the video-assisted group compared with 56% in the direct view group is 97 in each group for a corrected chi-squared test with 5% significance and 80% power.
Aim
Methods
Statistical analysis
Results
Discussion
According to the National Institute for Health Research,9 feasibility studies are used to estimate important parameters that are needed to design the main study. For example:
- standard deviation of the outcome
- willingness of participants to be randomised
- willingness of clinicians to recruit participants
- number of eligible patients, carers or other appropriate participants
- characteristics of the proposed outcome measure
- time needed to collect and analyse data
- to ensure recruitment, randomisation, treatment, and follow-up assessments all run smoothly.
measure, which is needed in some cases to estimate sample size
Crucially, feasibility studies do not evaluate the outcome of interest; that is left to the main study.
Teaching intubation is often a stressful time for both trainee and trainer. This is made considerably more comfortable when the view obtained by the trainee is witnessed by the trainer and accompanying nursing staff. When a successful intubation has been performed, all involved in the procedure have confidence that the ETT has been placed correctly. This increases confidence in trainee and trainer to allow instruction of intubation. If there is a higher success rate of intubation using VL, this is beneficial to any baby being intubated as there will be less hypoxia, stress and potential harm during attempts.
A weakness in the study could be that instruction given to the two groups during the procedure might have been different. This is a valid point, however it is one of the real advantages of the use of the video laryngoscope – clearer direction can be given with its use as all share the same view.
Concern over the use of a video laryngoscope for learning intubation would seem to be that trainees may be less successful at intubation if they are then faced with a laryngoscope with a direct view only. It has been shown that if trainees learn with video intubation, there is a tendency to be better at direct view subsequently.2 Previous concerns over the Storz C-Mac have been addressed. The distance from blade tip to light source/camera on the new handle is now 18mm on the 0 blade so it can be used for extreme preterm babies. Previously it had been 29.5mm, which meant that there had been difficulties in babies under approximately 800g. It has now been reduced to 19.5mm so can be used in smaller preterm babies (FIGURE 3). FIGURE 3 Storz C-Mac blades old (above) and new (below) showing the difference in distance from light source to blade tip.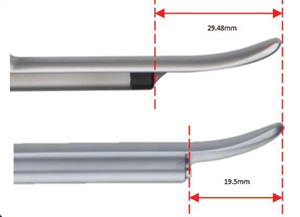
Conclusions
VL leads to improved success rates and increased team confidence around ETT placement during intubation. This is of utmost importance when the LISA technique is being performed due to the inability to check catheter placement with end tidal carbon dioxide monitoring and air entry.
In order to gain statistical significance a larger study will need to be undertaken. This feasibility study has shown that participants were willing to be randomised; clinicians were willing to recruit participants; the sample size for a future definitive trial is 97 in each group; the characteristics of the proposed outcome measure were highly skewed; the authors were able to estimate the time needed to collect and analyse data; recruitment could be estimated and randomisation was feasible; the intervention could be delivered and follow-up assessments were possible.
Or read this article in our
Tablet/iPad edition
- Intubation of newborn babies is a core skill for paediatric trainees.
- It is vital that the whole team is confident of catheter placement.
- There is a trend towards fewer attempts until successful intubation and increased team confidence when VL is used.
