

Speech and language therapy referrals following Bayley-III developmental assessment on ex-preterms
National Institute for Health and Care Excellence (NICE) guidance recommends multidisciplinary team input during enhanced developmental surveillance for up to two years corrected age in ex-preterm children. However, achieving this may be challenging because of resource constraints. There is a lack of nationally comparable data on neonatal follow-up programmes and outcomes. This article describes a service evaluation of a local neonatal follow-up programme and the role of quality assurance while aspiring to meet NICE recommendations.
Sagarika Ray
MBBS, MSc, FRCPCH
Consultant Neonatologist
Department of Neonatal Medicine,
The Shrewsbury and Telford Hospital
NHS Trust
sagarika.ray@nhs.net
Preterm infants have been recognised as a population with a heightened risk of developing linguistic disorders and early language delays.1,2 Language delay at two years proved to be a sensitive marker for different developmental problems and adequate early intervention requires clear distinction between expressive, receptive-expressive, and other associated neuro-developmental problems. Thus, a ‘wait and watch’ approach is not justified in young children.3 Early and timely referral to speech and language therapy (SLT) is desirable.
Guidance from Developmental Follow-up of Children and Young People Born Preterm (NICE, NG72)4 recommends multidisciplinary team (MDT) input during enhanced developmental surveillance up to two years of corrected age in the form of a neonatologist or paediatrician with an understanding of neonatal care and child development, and at least one of an occupational therapist, physiotherapist and/or speech and language therapist. However, multidisciplinary input during face-to-face visits may not be achieved in some settings due to resource constraints.
Current pathway in Shropshire
The British Association of Perinatal Medicine (BAPM) and Royal College of Paediatrics and Child Health (RCPCH) Working Group on Classification of Health Status at Two Years as a Perinatal Outcome (2008) recommended that all neonatal services should plan to develop their follow-up service to include a formal developmental assessment using the Bayley Scales of Infant and Toddler Assessment Third Edition (Bayley-III). The literature reveals that cognitive and languages scales of the Bayley-III are a useful instrument for early diagnosis of language disorders and can also discriminate more severe forms.5
The current care pathway in Shropshire involves ex-preterm children undergoing a structured developmental assessment in the form of Bayley-III. If language scores indicate a difficulty, the children are subsequently referred to SLT services.
This set-up is similar in various regions throughout the UK. A service evaluation was undertaken by the neonatal services and SLT services within Shropshire to evaluate the current care pathway and check for quality assurance and outcomes, measure parental engagement, and identify any service capacity issues.
Methodology
Retrospective data over a 2.5 year period (May 2016 to October 2018) were collected from electronic patient records of eligible preterm children undergoing a Bayley-III assessment at two years corrected age. If mild, moderate or severe difficulties in receptive or expressive language skills were identified, they had been referred to SLT services. The SLT team had then triaged the referral and undertaken an initial assessment through play, resulting in a subjective assessment based on experience. For the purposes of this project, the SLT assessments were also categorised into mild, moderate, or severe difficulties based on the proposed time of recall for a subsequent SLT appointment (TABLE 1).
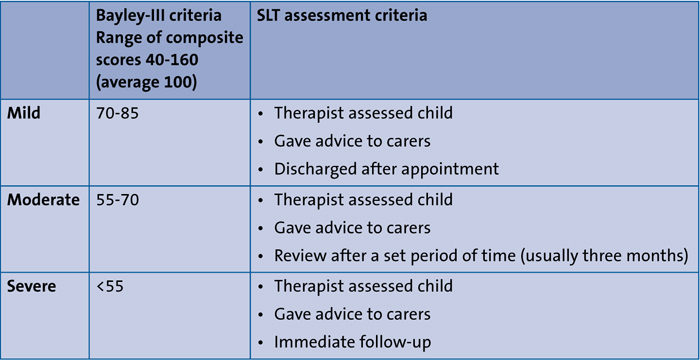
TABLE 1 Categorisation of severity of language (receptive and expressive) skills through Bayley-III criteria and SLT assessment.
Results
Nineteen children were referred to SLT, of which one moved out of area. Good parental engagement was evidenced by 72% uptake of SLT appointments. The children were seen by SLT within 3-4 months of the referral. There was a good level of correspondence between the Bayley-III assessments and post-referral SLT assessments in 78% of nine children for whom complete data were available (TABLE 2). The two children assessed as having mild difficulty through Bayley-III scores but moderate by SLT, were still referred as per pathway and did not miss any scope of SLT intervention, which is reassuring. Seventy-three per cent of children are still having ongoing SLT input. Of interest, the mean age of SLT referral for children following Bayley-III assess-ment was two years and four months as compared to three years for a sample of children from the current pre-school waiting list.
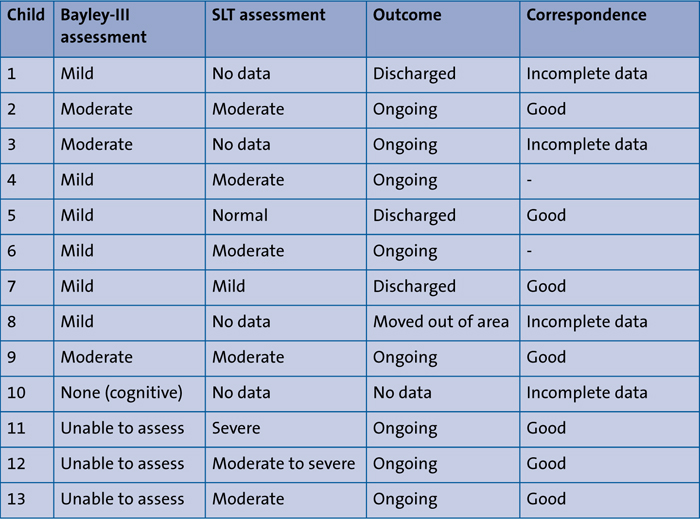
TABLE 2 Outcomes of language difficulties (categorised as mild, moderate, or severe) following Bayley-III and SLT assessments in 13 children who underwent assessment.
Although the sample size is modest, the results (summarised in TABLE 3) reveal interesting implications for practice. Most children in this cohort are still having ongoing SLT input, hence indicating that the correct categories of children are being referred. Children in this cohort were referred eight months earlier from Bayley-III assessments, thus enabling timely intervention. Good correlation between Bayley-III and SLT assessments and SLT referral times indicate that the current service in our local setting is acceptable at present. However, given that language delay at two years can be a sensitive marker for developmental problems and the wait and see approach is not justified,3 SLT presence during enhanced developmental surveillance as per the NICE recommendation is welcome as it may speed up the process for these children to access SLT intervention.
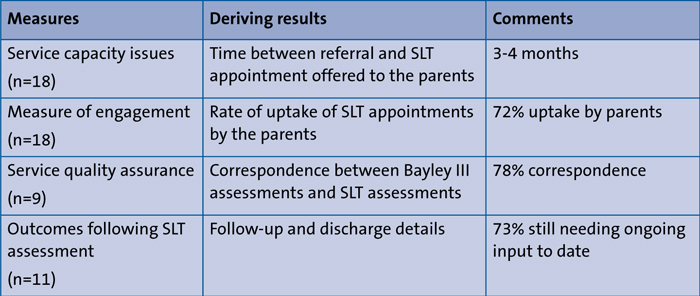
TABLE 3 A summary of the results.
Discussion
The association of preterm birth with developmental issues is well recognised. Hence, the inclusion of a two-year assessment for high risk infants was included in the Toolkit for Neonatology from the Department of Health.6 However, there is paucity of reliable and comparable national data in the UK with regards to the quality of the service and outcomes of neonatal follow-up programmes, due to regional variations in provision of this service. Two-year follow-up is considered a measure of neonatal outcome and is a standard of care that is monitored through the National Neonatal Audit Programme (NNAP). Data captured through NNAP is dependent on UK-wide data entry through individual units and this may limit data collection and analysis of medical two-year follow-up due to instances of outcomes being ‘not determinable’ due to missing data. The NNAP also demonstrates the wide variation in provision of follow-up and data capture, as partial data is just available for 60% of these high-risk children,7 thus highlighting the need for more robust and representative data from neonatal follow-up programmes throughout the UK.
It is also noteworthy that the recent NICE guidance does not mention the commonly used validated structured developmental assessments, such as the Bayley-III and Griffiths assessments, but does recommend the use of a MDT approach to enhanced developmental surveillance, along with some assessments and questionnaires that are not routinely used in current UK practice. This may further contribute to the challenge of nationally comparable data on neonatal follow-up programmes. Classification of mild, moderate, and severe impairment from the NNAP impairment category datasets are derived from qualitative data and not from the standardised developmental assessments.8
The other area of focus is access to services once a need for referral is identified following an assessment. Although our local service evaluation indicated early and timely referral to SLT services was possible with the correct category of children being referred, the availability of services and resources can vary widely throughout the UK. As there are no national waiting time targets for SLT services, it is up to local commissioners to ensure children can access services in a timely manner.9 The Bercow: Ten Years On (2018) national report found more than a third of surveyed parents waited over a year to access SLT services, although these referrals were not exclusively from the ex-preterm population.10
Conclusion
This county-wide service evaluation revealed that the current setting was acceptable in terms of the right category of children being referred to SLT, good correspondence between Bayley-III and SLT assessments, and high parental engagement. Sharing our local findings and implications for practice with a wider audience highlights the importance of individual neonatal services ensuring quality assurance of their local neonatal follow-up programme with regards to appropriate and timely referrals of children to therapy services, especially where immediate achievement of NICE recom-mendations may be challenging due to resource constraints. MDT input is always welcome for the holistic assessment of the child and it may be more crucial in the context of the NICE guidance where other assessment methods and questionnaires are recommended. Our data has demon-strated that with structured assessments, such as the Bayley-III, it is possible to identify and make appropriate referrals in a timely fashion, while aspiring to meet NICE recommendations.
Acknowledgements
The author would like to thank Alison Black, Speech and Language Therapist, Shropshire Community Health NHS Trust, for providing some of the data included in this service evaluation.
Or read this article in our
Tablet/iPad edition
- The outcomes of speech and language therapy (SLT) referral following developmental follow-up of children born preterm are explored.
- There is a paucity of comparable national data with regards to the quality assurances and outcomes of neonatal follow-up programmes due to regional variations in provision of this service.
- A county-wide service evaluation revealed that the current setting was acceptable and highlighted the importance of quality assurance of local neonatal follow-up programmes.
- The presence of SLT input at developmental assessments as per NICE recommendation is warranted as it speeds up the process for these children to access SLT intervention.
