

Haemorrhagic shock revealing a neonatal Wilms’ tumour
This case report describes a neonatal Wilms’ tumour in a 20-day-old boy that was revealed in unusual circumstances. The infant was admitted to the intensive care unit with haemorrhagic shock and an abdominal mass. Following transfusion and stabilisation, scans showed a left kidney tumour with haemorrhage. The infant underwent a left ureteronephrectomy with reduced-dose chemotherapy. At the six-year follow-up examination he was free of recurrence and metastases.
Fatma FitouriMedical Doctor
fitfatma@yahoo.fr
Yasmine Houas
Pediatric Surgeon
Nizar Sassi
Pediatric Surgeon
Sondes Sahli
Medical Professor
Mourad Hamzaoui
Medical Professor
Department of Pediatric Surgery A, Children’s Hospital, University of El Manar, Tunis, Tunisia
The case report
A 20-day-old boy was admitted to the intensive care unit for haemorrhagic shock. He was hypothermic, his heart rate was 145 beats/min and his blood pressure was 40/20mmHg. A physical examination revealed cutaneous paleness and a large left-sided abdominal-pelvic mass (FIGURE 1). Laboratory investigations revealed anaemia with a haemoglobin level of 2g/dL and thrombocytopenia with a platelet count of 29x109/L.

FIGURE 1 Abdominal distension in the 20-day-old infant.
Haemorrhagic shock is a life-threatening condition of reduced tissue perfusion as a result of inadequate delivery of oxygen. It is important that haemorrhagic shock is identified and appropriately managed without delay. The newly-born child was transfused with 20mL/kg of O-negative, non-cross matched blood and fresh frozen plasma.
Following transfusion and stabilisation, an abdominal ultrasound and a computed tomography scan revealed a multi-septate cystic left kidney tumour (FIGURE 2) measuring 90x55x55mm. Primary surgery was indicated. A transverse laparotomy showed a fissured kidney tumour with the presence of blood in the peritoneal cavity (haemoperitoneum). A total uretero-nephrectomy was performed. The mass weighed 195g.
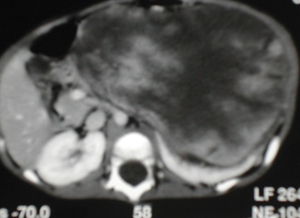
FIGURE 2 A computed tomography scan revealing a multi-septate tumour of the left kidney.
Histological examination revealed a stage 2 SIOP (International Society of Paediatric Oncology) Wilms’ tumour with blastemal cells but without lymph node involvement.
Reduced dose chemotherapy (vincristine and actinomycin D) was administeredfor 33 weeks. The patient was free of recurrence and metastases at the six-year follow-up examination.
Discussion
Neonatal tumours are rare, with an incidence of one in 12,500-27,500 live births and comprising 2% of childhood malignancies.1 Seven per cent of neonatal tumours are renal.2,3
Abdominal masses in newborn babies occur in 0.2-0.6% of live births and the majority of them are related to the urogenital tract.4,5 Wilms’ tumour is the most common paediatric renal tumour and the clinical features include a palpable abdominal mass,2 arterial hypertension and haematuria.4 Haemorrhagic shock is an unusual presentation. About 16% of these tumours are diagnosed antenatally by ultrasonography as a renal mass or during investigation for maternal polyhydramnios, hydrops fetalis or other congenital anomalies.6 In this case, the mother did not have an antenatal scan.
Haemodynamic stability is necessary before any surgery hence the vascular filling, blood transfusion and fresh frozen plasma administered in this case.
Primary radical ureteronephrectomy is the main surgical treatment. In neonatal Wilms’ tumour no effective treatment guidelines have been established. Chemotherapy is rarely indicated in neonates, reserved only for high stage tumours or high-risk histology.2
Classic Wilms’ tumors are triphasic and histologically composed of epithelial, blastemal, and stromal elements.7 Stage 1 and 2 Wilms’ tumours frequently have a good prognosis.
Conclusion
Although extremely rare, Wilms’ tumour should be systematically considered when renal tumours are encountered in a newborn baby. Haemorrhagic shock is an exceptional finding in Wilms’ tumour. It requires urgent care and management needs to be coordinated by a multi-disciplinary team.
Parental consent
The authors received written consent to publish this report from the patient’s parents.
Or read this article in our
Tablet/iPad edition
- Wilms' tumour (also called nephroblastoma) is a malignant tumour of the kidney. Likely symptoms include swelling of the abdomen.
- Wilms’ tumour is the most common childhood abdominal malignancy but neonatal Wilms’ tumour is very rare.
- Despite its rarity, Wilms’ tumour should be considered in cases of neonatal haemorrahagic shock.
