

Management and outcome for babies born with an exomphalos
Exomphalos is an abdominal wall defect that is commonly associated with other abnormalities and/or chromosomal anomalies; however, there is limited information about the incidence of co-morbidities, management strategies and outcomes in this population. This retrospective case review describes key outcomes for 29 infants with exomphalos admitted to a surgical neonatal intensive care unit over a nine-year period.
Sarah Louise WilliamsonMBChB(hons), MRCPCH
Paediatric Registrar
sarahlouise.williamson@nhs.net
Louise Lawrence
RN, BSc
Clinical Nurse Specialist in Neonatal Surgery
Anthony Lander
Phd, FRCS (Paeds), DCH
Consultant Paediatric Surgeon
Shree Vishna Rasiah
BMBS, MRCPCH
Consultant Neonatologist
Birmingham Women’s and Children’s NHS Foundation Trust
Exomphalos (omphalocele) is a congenital abnormality arising due to a defect in the anterior abdominal wall of the umbilical ring.1 The defect results in herniation of the abdominal contents so that they protrude outside the abdominal cavity within a sac surrounding the umbilical cord. The sac consists of three separate layers: the amnion and perito-neum separated by Wharton’s jelly, which protect the intestine and theoretically allow the bowel to function normally.1 The reported prevalence in the UK is 3.8 per 10,000 births.2 Among these 3.8 cases:
- exomphalos is an isolated finding in 1.4 cases
- 1.2 cases have other associated abnormalities
- 1.2 cases have chromosomal anomalies.2
Associated abnormalities have been shown to influence long-term survival. One-year survival in isolated anomalies is reported as 91%, compared with 81% in multiple abnormalities and 27% if associated with chromosomal anomalies.3
Exomphalos is categorised as major or minor. Exomphalos major is defined as an abdominal wall defect >5cm and/or the liver is inside the sac (FIGURE 1). In exomphalos minor the defect is <5cm and only contains intestines.4
There is no national guideline or current national consensus on how to manage exomphalos major. It can be managed, conservatively, consisting of delayed surgical closure of the abdominal wall defect at approximately one year of age after full epithelisation of the sac.5 This is achieved by applying a topical anti-microbial agent. Bauman et al’s systematic review in 20165 found that conservative management is associated with lower mortality and shorter duration of enteric feeding. Exomphalos minor is largely managed with primary repair.1

FIGURE 1 Day 1 exomphalos major showing herniation of the bowel and liver through the umbilical ring into the base of the umbilical cord.
Methods
The aim of this retrospective review was to share our experience of managing neonates with exomphalos and to describe the key outcomes for infants and their families. We carried out a retrospective case note review of all infants diagnosed with exomphalos and admitted to our surgical neonatal intensive care unit (NICU) in the West Midlands (which works closely with a neonatal surgical unit on another site). We identified infants over a nine-year period between 1 April 2009 and 31 March 2018. Data were collected from BadgerNet electronic patient records and paper notes.
A surgical neonatal unit’s experience
Birmingham Women’s and Children’s NHS Foundation Trust (BWC) has a 41-bed tertiary NICU receiving approximately 2,000 admissions per year. It is the regional referral centre for complex congenital abnormalities but exomphalos by itself is not an indication to deliver at BWC, although these babies should ideally be delivered in a NICU. Reviewing the unit’s data revealed that over the last nine years 29 infants were admitted with a diagnosis of exomphalos. Of these, 17 cases were classified as exomphalos major (59%) and 12 as exomphalos minor (41%). The mean gestation at birth for these infants was 36 weeks’ (range = 28-40 weeks’ gestation), weighing on average 2,965g (range 1,130-4,730g). Sixteen of the infants were male (55%).
Following delivery eight infants (28%) required intubation and ventilation, and five (17%) required inotropic support. The majority of these infants had a diagnosis of exomphalos major, only one infant with exomphalos minor required intubation and ventilation at birth; however, it was born prematurely at 30 weeks’ gestation.
Post-delivery it is best practice to assess for associated congenital anomalies, due to the high incidence of associated structural malformations. Echocardiogram was performed in 24 infants (83%) to look for associated cardiac anomalies. Structural anomalies were identified in 17 infants (59%); four infants were felt to have significant anomalies (TABLE 1). Cranial imaging was performed in 22 infants (76%) and 24 (83%) underwent renal imaging. Excluding cardiac anomalies, other congenital anomalies were identified in 10 infants (34%), most commonly musculoskeletal (six infants), gastro-intestinal (four infants), and ear, nose and throat (three infants) (TABLE 2). An underlying genetic diagnosis was identified in 10 infants (34%), most commonly being Beckwith-Wiedemann syndrome (n=8). One infant had maternally inherited 3q28 deletion of uncertain significance and one had 22q11.2 deletion.
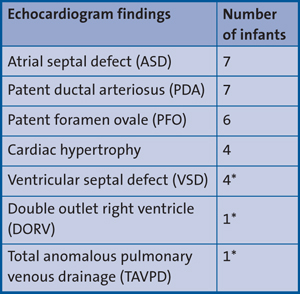
TABLE 1 Echocardiogram findings. An echocardiogram was performed in 24 infants. Structural anomalies were identified in 17 infants; four infants were felt to have significant anomalies. *Cardiac lesions deemed significant.
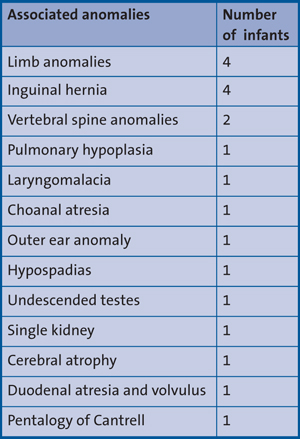
TABLE 2 Associated anomalies (excluding cardiac anomalies). Other congenital anomalies were identified in 10 infants.
The overall mortality was 21% (n=6); all of these infants had a diagnosis of exomphalos major. Their characteristics are shown in (TABLE 3). Two had an under-lying genetic diagnosis and three had significant associated congenital anomalies. Five infants who died were born preterm (28-36 weeks’ gestation). The time of death ranged from the day of birth to two years of age.
Of the 11 surviving infants with exomphalos major, all underwent initial conservative management with anti-microbial dressings and delayed surgical closure following full epithelialisation of the sac. Discharge home was on average 38 days of age. To date, eight of these infants have undergone definitive surgery at an average age of 39 months (range = 12-124 months). The remaining three infants remain under review.
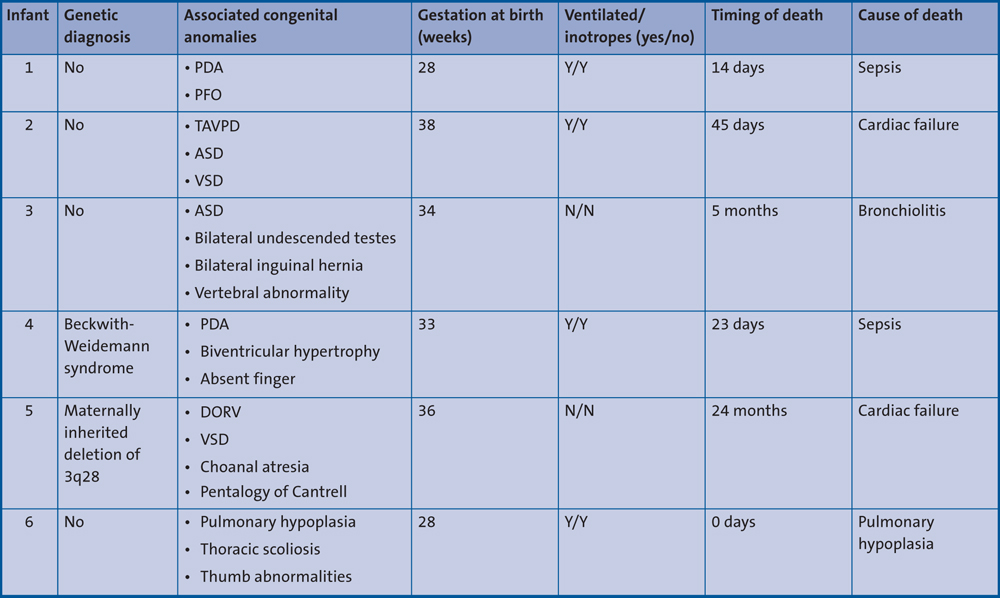
TABLE 3 Characteristics of the six infants with exomphalos major that died. Key: PDA = patent ductal arteriosus, PFO = patent foramen ovale, TAVPD = total anomalous pulmonary venous drainage, ASD = atrial septal defect, VSD = ventricular septal defect, DORV = double outlet right ventricle.
Primary closure was performed in 10 infants with exomphalos minor prior to discharge (83%). The remaining two infants had minor defects and were discharged home without surgery. Surgery was performed in one if these infants at four years of age. The other infant is still under review.
There is no national consensus on how to manage exomphalos in the UK and it is difficult to compare outcomes at BWC with other units due to the lack of consensus in management and a limited availability of data.
Clinical pathway following antenatal diagnosis
All parents of infants with an antenatal diagnosis of exomphalos are offered antenatal counselling with a multi-professional team including a consultant paediatric surgeon, neonatologist and surgical outreach nurse. For management of exomphalos, BWC follows the neonatal network guidelines published by the Staffordshire, Shropshire and Black Country Neonatal Operational Delivery Network.4
At delivery a plastic clamp is placed on the umbilical cord >10cm away from where the normal cord starts. This is to avoid bowel injury.4 The baby’s legs and abdomen are then placed in a sterile plastic bag, a large bore nasogastric tube is inserted and the baby is commenced on prophylactic broad spectrum antibiotics. On admission to the neonatal unit a thorough assessment identifies any associated congenital anomalies. Genetic analysis is offered if this has not been performed prenatally. It is important to be aware of the association between Beckwith-Wiedemann syndrome and profound early neonatal hypoglycaemia.1 Management is then focused on nutrition, fluid balance and replacement of fluid losses.1 Feeds are introduced and increased as tolerated. Mothers are encouraged to breastfeed or express breast milk.
After delivery, all infants are assessed by the Birmingham Children’s Hospital Surgical Outreach Service and if defined as an exomphalos major they are managed conservatively, avoiding the need for transfer to the regional surgical centre.
The exomphalos sac is dressed with a topical antimicrobial agent, gauze and crepe bandage (FIGURES 2-4). First line topical treatment at BWC is Activon Manuka Honey. The dressing is changed twice weekly. The baby is weighed at dressing changes and has weekly clinical photography and swabs of the sac sent for microbiological assessment. It is essential to avoid rupture or damage to the protec-tive sac as this may require emergency surgery. Parents are taught how to change the dressings and, once competent, they are discharged home with support from the surgical outreach service and local paediatric community nurses. Dressing of the exomphalos sac is continued until full epithelialisation is achieved (FIGURES 5-7).
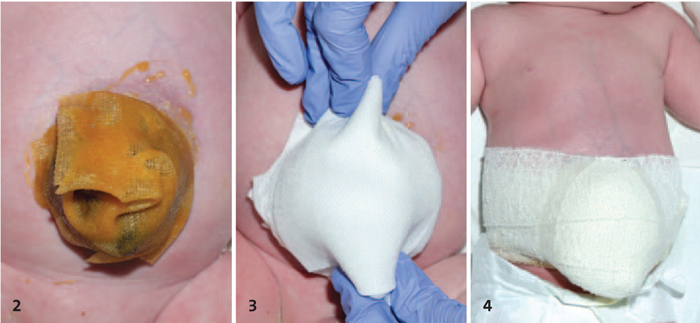
FIGURE 2-4 The exomphalos sac is dressed with gauze and Manuka honey. A crepe bandage is applied.

FIGURE 5-7 Dressing of the exomphalos sac is continued until full epithelialisation is achieved.
Conclusion
Exomphalos major can be effectively managed with conservative management and delayed surgical closure. Daily support from the surgical outreach team allows these infants to be managed on the NICU, avoiding unnecessary transfer to the tertiary surgical centre.
The British Association of Paediatric Surgeons Congenital Anomalies Surveillance System (BAPS-CASS) study6 is a prospective observations study to assess the incidence, comorbidities, management and outcomes of infants born with exomphalos in the UK and Ireland. BWC has submitted data to this study with the hope that it will lead to a greater consensus in management in the future.
Our experience suggests that infants with a diagnosis of exomphalos major and associated congenital or genetic anomalies are at increased risk of mortality, especially if born premature or if they require ventilatory and/or inotropic support in the immediate postnatal period. This review has enabled us to give parents more detailed information during antenatal counselling.
Parental consent
The authors received permission from the patients’ parent(s) to publish the images in this article.
Or read this article in our
Tablet/iPad edition
- Exomphalos major can be effectively managed with conservative manage-ment and delayed surgical closure.
- Infants with exomphalos major and associated congenital or genetic anomalies are at increased risk of mortality, especially those born premature or requiring ventilatory and/or inotropic support.
- This review enables us to give parents more detailed information about prog-nosis, management techniques and outcomes during antenatal counselling.
