

Swaddling the newborn infant: then and now
This article discusses the custom of swaddling an infant during the first months of its life from ancient to modern times, reaching the conclusion that swaddling is a practice in modern infant care that should be abandoned forthwith.
Peter M. DunnMA, MD, FRCP, FRCOG, FRCPCH Emeritus Professor of Perinatal Medicine and Child Health, University of Bristol
p.m.dunn@bristol.ac.uk
Part I: Then
The custom of swaddling an infant during the first months of its life was both ancient and widespread, especially in cooler climates. It consisted of compressing the infant’s body into a mummy-like mould using a system of tight bandages (FIGURE 1).

FIGURE 1 A swaddled infant from the facade of the Foundling Hospital in Florence (Andrea Della Robbia (1435-1525).
Greek physician Soranus of Ephesus (AD 98-138)1 gave a detailed description of the practice, mentioning the orthopaedic reasons for swaddling in the following passage:
“Rather one must mould every part according to its natural shape, (and) if something has been twisted during the time of delivery, one must correct it and bring it into its natural shape.”
Galen of Pergamum (AD 129-200)2 made similar recommendations adding that swaddling helped to protect the delicate skin of the newborn baby. He wrote:
“But when the baby is born, it is necessarily going to come in contact with cold and heat and with many bodies harder than itself. Therefore it is appropriate that his natural covering should be best prepared by us for exposure.”
And he also added a warning:
“In little children... their cries and screams... mean something is annoying them... It may be that they want warmth when they are cold, or cool when they are hot, or they are in discomfort from their swaddling bands, for even those are a burden... I have also noticed that his cot and all his wrappings were too dirty and the infant himself dirty and unwashed, and I have ordered him to be bathed and that she should change his napkins for clean ones, and when these things were done the infant has stopped kicking and has settled off in a long sleep.”
Some 1,300 years later a book on children by Paulus Bagellardus3 gave almost identical instructions to those of Soranus on how to swaddle an infant:
“After this, she should cover the infant’s head with a fine linen cloth after the manner of a hood. Then secure a soft linen cloth and with the infant placed on the midwife’s lap in such a way that its head is toward her feet and its feet rest upon her body, the midwife should roll it in the linen cloth, after it has been bathed, wrapping its feet. First with its arms raised above, she should warp its breast and bind its body with a band, by three or four windings. Next the midwife takes another piece of linen or little cloth and draws the hands of the infant straight forward towards the knees and hips, shaping them evenly, so that the infant acquires no humpiness. She then, with the same assisting band, binds and wraps the infant’s arms and hands, all of which will be correctly shaped. Then she should turn the infant over on its breast with its back raised upward and, taking hold of the infant’s feet, make its soles touch its buttocks to the end that its knees might be properly set. Thereupon she should straighten the infant’s legs and with another band and little cloths bind and wrap up the hips. Next take the entire infant and roll it in a woollen cloth or after our manner in a cape lined with sheep skins; and this in winter, but in summer a linen cloth .”
The practice remained popular in Europe until well into the 18th century (FIGURE 2). Francois Mauriceau (1637-1709),4 a famous French accoucheur (male midwife), again recommended that:
“To prevent a child’s growing crooked or awry or lame, the nurse must swaddle its body in a straight situation, equally extending the arms and legs.”

FIGURE 2 Swaddling in the 17th century.
However, he added that:
“While all other animals have their bodies free, without the trouble of coverings, so they easily discharge themselves of their excretements... it is not the same with infants who (being bound and swath’d with swathes and blankets, as we are forced, to give them a straight figure only suitable for mankind) cannot render their excretements.”
Felix Wurtz of Basel (1515-1575) was the first to sound a serious warning against swaddling. In his book on children (1563)5 he wrote:
“I have seen children born straight, yet became lame and crooked, and could not be healed straight again; their mothers or nurses... will not leave the birth as God hath created it, will have their children yet handsomer, by binding them straighter to their thinking, tye and bind them more crooked, doing it so hard, which maketh the child unquiet... when children are bound straight with strong binding then they usually grow crooked; and none will grow more straight in his body, than those which are laid free and loose with their hands and feet: Therefore my advice is, not to use any curiousities at the laying and binding your children.”
English philosopher John Locke (1632-1704) also rejected swaddling in his book Some Thoughts Concerning Education (1693) but it was Dr William Cadogan of Bristol (1711-1797) in his Essay upon the Nursing and Management of Children from Their Birth to Three Years of Age (1748)6 who made the strongest plea for the universal abandonment of swaddling:
“Besides the mischief arising from the weight and heat of these swaddling-cloathes, they are put on so tight, and the child is so cramped by them, that its bowels have not room, nor the limbs any liberty, to act and exert themselves in the free easy manner they ought. For limbs that are not used will never be strong, and such tender bodies cannot bear much pressure: the circulation restrained by the compression of any one part, just produce unnatural swellings in some other; especially as the fibres of infants are so easily distended. To which doubtless are owing the many distortions and deformities we meet with everywhere.”
The British male midwife William Smellie (1697-1763)7 also made an important observation in 1752 on the impact of tight binding on the respiration of an infant:
“I have been called several times, where I found the uneasiness of the children proceeded from too tight dressings; and by observing this circumstance in time, the danger was prevented by dressing them looser... About two years ago, I was called to see a child, on the fourth day after delivery, and was told that it heaved, and had an oppression at its breast. The nurse undressed the child; and the clothes did not seem tight, but I observed the bandage on the navel appeared very tight. This I ordered to be unrolled; and plainly perceived that it was the cause of the disorder; for the child immediately breathed with greater freedom, and did very well .”
Jean Jacques Rousseau, the philospher of Geneva (1712-1778) wrote in 1762:8
“The child had hardly left the mother’s womb, it had hardly begun to move and stretch its limbs, when it is given new bonds. It is wrapped in swaddling bands, laid down with its head fixed, its legs stretched out, and its arms by its side; it is wound round with linen and bandages of all sorts so that it cannot move... Whence comes this unreasonable custom?... A child unswaddled would need constant watching; well swaddled it is cast into a corner and its cries are ignored. It is claimed that infants left free would assume faulty positions and make movements which might injure the proper development of their limbs. This is one of the vain rationalisations of our false wisdom which experience has never confirmed.”
Dr William Heberden (1710-1801), a distinguished English physician, added his voice to the criticism of swaddling:
“Let them take example from nature and follow in her steps.”
The great Swedish paediatrician, Nils Rosen, added his authority to the criticism of swaddling, writing in 1776:9
“The most approved practice would be never to swaddle children, which physicians have demonstrated by convincing arguments... was a full grown person obliged to be thus swaddled, would he not think it a great hardship? But we seem to have no compassion on our innocent children.”
How correct was Rosen in his assessment. It is distressing even to contemplate the suffering of infants in their tight swaddling, unable to move and exercise, to control their temperature, to breathe easily especially after feeds, and lying excoriating in their excreta often for long periods. Apart from the suffering, there can be little doubt that swaddling made a major contribution to the very high infant mortality of those early days.
As William Cadogan also wrote:6
“The mother who has only a few rags to cover her child loosely, and little more than her own breast to feed it, sees it healthy and strong, and very soon able to shift for itself: while the puny infant, the heir and hope of a rich family, lies languishing under a load of finery that overpowers his limbs, abhorring and rejecting the dainties he is crammed with, till he dies a victim to the mistaken care and tenderness of his fond mother.”
Gradually the practice of swaddling declined in Europe during the 17th and 18th centuries.
Part II: Now
Let us now fast forward 200 years to the second half of the 20th century. Swaddling seemed to have become a historical memory. However a vestigial remnant of it remained in the form of the umbilical binder. A crepe bandage around the abdomen was applied at birth with a view to protecting the umbilical stump from infection until it desiccated and fell off a few days later. In fact I discontinued the use of an umbilical binder in the maternity hospital where I was working as a registrar in 1960, as in my view it retarded desiccation and healing of the umbilical stump and encouraged infection. Furthermore, and more importantly, Professor John Emery (who had trained in Bristol) reported in 1967 two neonatal deaths that he attributed to tight umbilical binders10 that, following a feed, had led to upward displacement of the diaphragm and obstructed respiration. This was the same problem previously described by William Smellie in 1752,7 yet umbilical binders still continue to be used around the world.
Back in 1959 I commenced a 10-year study on the aetiology of congenital postural deformities and, in particular, congenital dislocation of the hip (CDH).11 I was able to show that quite gentle pressure, when maintained on the rapidly growing fetal
ip joint, especially if the thighs were persistently adducted as in a case of frank breech presentation (FIGURE 3), might lead to dislocation.12-14 I was also able to show that some 2% of newborn infants in the UK had unstable or dislocated hips at birth (FIGURE 3), although many of the dislocatable hips would stabilise in the days or weeks following delivery. As a result, prior to the institution of neonatal screening and early treatment, the incidence for CDH at 2-3 years of age in the UK was around 1% or approximately 7,000 new cases each year.
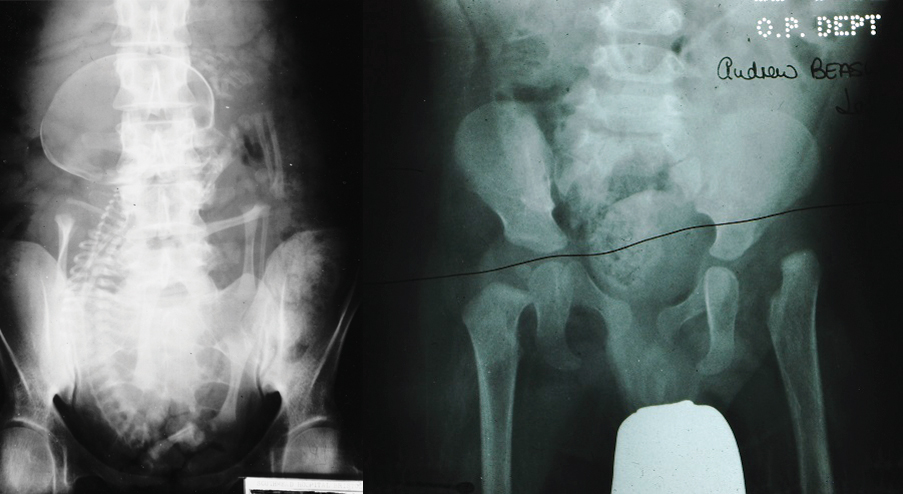
FIGURE 3 Left: Frank breech presentation with legs flexed and adducted. Right: Congenital dislocation of the left hip at the age of six months.
Newborn infants, when unconstrained, adopt a posture in which the hips are flexed and abducted away from the line of the body. This is infact the posture we use to treat infants diagnosed with CDH at birth. Abduction of the hip drives the head of the femur, through the anchor of the Y-shaped ligament of Bigelow (iliofemoral ligament), deep into the acetabulum.15
Early in my study of the aetiology of CDH11 I had become interested in the great variation in the incidence of this condition around the world. It was clear that while CDH was rare in many tropical countries, the incidence rose progressively as one moved into colder climates, reaching an incidence as high as 5-6% among Lapplanders.
Since 1959 I have studied the way newborn infants are nursed by their mothers or carers. At first my knowledge was derived from the study of countless copies of the National Geographic magazine but later on by personally visiting some 80 countries around the world and seeing for myself. I now have an extensive collection of photos on how babies are nursed (FIGURE 4).
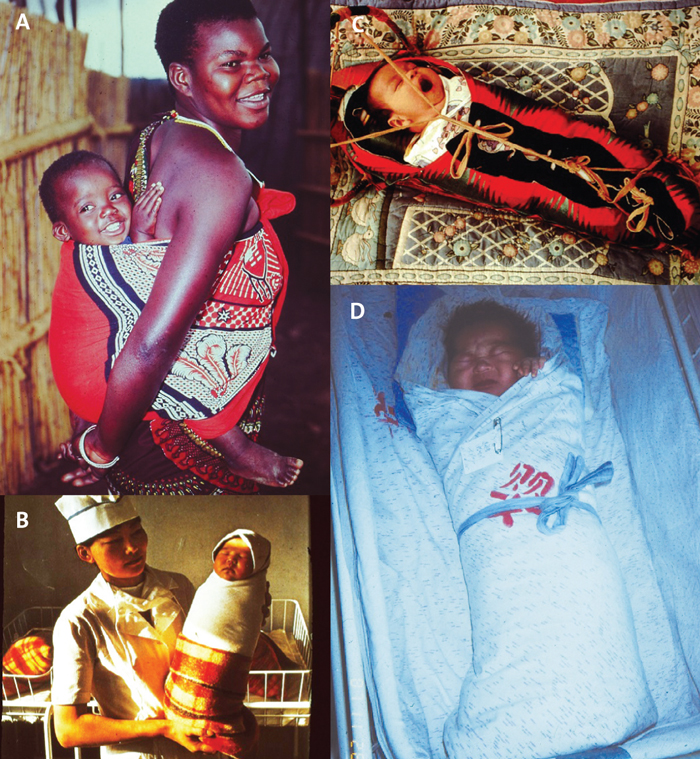
FIGURE 4 (A) A baby in Swaziland nursed across his mother’s back with his legs abducted. In South Africa, CDH is extremely rare. (B) An infant tightly wrapped in Outer Mongolia. (C) A Native American baby in northern Canada in a papoose – a birch bark cradle permitting ready mobility in a hunter-gatherer society. (D) An infant tightly wrapped in blankets in China. The last three infants have their legs inevitably extended and adducted at the hip; such populations have a high incidence of CDH.
Another factor appearing to influence the incidence of CDH is the season of birth. Reports from many countries, including the UK, have noted an increase in the incidence of CDH, often a doubling, among infants born in the winter months. It has been suggested the colder weather leads to the use of heavier clothing and blankets, which in turn restrict the infant’s free movement and favour adduction of the thighs especially when the infant is lying on its side.11
It is of interest that de novo infantile dislocation of the hip may occur as a complication of infants with congenital spastic diplegia (Little’s disease) in which muscle spasm holds and maintains the legs in extension and tight adduction. This again lends support to the observation that the hip joint is vulnerable to dislocation when the legs are held persistently in adduction.
Nor is it just in remote lands that there is still a problem with swaddling. In many countries birthing now mainly takes place in hospital and, for a variety of reasons, babies may be nursed separately from their mothers only being united at intervals for feeding. To ease transfer the babies are often firmly wrapped in blankets. This is known as ‘bundling’ but is not that different from swaddling in terms of its effect on the infant.
Since the 1990s some doctors have promoted swaddling suggesting that not only do infants sleep better and cry less,16 but that this method of nursing may protect them against cot deaths. However, research undertaken by Professor Peter Fleming and his colleagues has shown that swaddling may actually significantly increase the risk of the sudden infant death syndrome.17,18
In my view, swaddling is a practice in modern infant care that should be abandoned forthwith. Not only does it increase the incidence of the crippling deformity, CDH, but also it may lead to de novo infantile dislocation of the hip. It can prevent the infant from exercising its muscles and joints. Swaddling may also rob the infant of its ability to control its temperature; hyperthermia, as well as hypothermia, can prove fatal.19 In addition, swaddling, especially after feeds, may hinder respiration. It may lead to regurgitation, inhalation and pulmonary infection and it is feasible that it may be responsible for later psychological problems. This latter point is fertile ground for further research. Luckily our memories are not good in the first year of life but which of us as adults would survive without psychological damage if we were severely constrained in a way not dissimilar to the use of a straight jacket for a period of several months.
Nowadays, healthcare staff may use bundling prior to under-taking some procedures on the neonatal unit (eg, prior to giving medication, taking blood, to aid lumbar puncture, etc) and it is my view that this short-term bundling would not be harmful. However, outside of these circumstances swaddling should be universally discarded as a most undesirable and dangerous practice.
Or read this article in our
Tablet/iPad edition
