

Phototherapy at home for the treatment of neonatal jaundice: a patient-centred pilot project
Phototherapy is a well-established procedure and the mainstay of treatment for significant neonatal jaundice. Usually, phototherapy is delivered in hospital, typically requiring a hospital stay of a few days. This article describes a pilot project to introduce phototherapy for the management of neonatal jaundice in clinically stable preterm and term infants with haemolytic disease of the newborn using a phototherapy blanket at home.
Devangi ThakkarNeonatal Trainee
Amit Verma
Neonatal Trainee
Sriparna Kar
Sarah Brookman
Christian Catalano
Jessica Hill
Lyndon Wells
Paediatric Trainees
Malgorzata Radomska
Neonatal Associate Specialist
Neonatal Unit, Evelina London Children’s Hospital, Guy's and St Thomas' NHSFT
Background
In 1958, Richard Cremer published Influence of Light on the Hyperbilirubin-aemia of Infants,1 which documented the effects of natural sunlight and artificial light on lowering bilirubin levels in infants. Since then, the practice of treating neonatal jaundice with phototherapy has become well established, researched, recognised and recommended by experts.2 Modern phototherapy machines use halogen bulbs, light emitting diodes (LED), fluorescent light or a combination of all three, in addition to blankets that contain fibre optics to increase skin exposure to light. Combination lights are the most effective because they deliver the intensity of halogen spotlights and the use of LEDs cuts down on excessive heat generated during a session.
Fibre optic phototherapy blankets – glowing cushions or biliblankets – are the most ‘friendly’ form of treatment. Therapy can continue during cuddles and breast-feeding. It is also better tolerated by babies who become unsettled if undressed and exposed to the overhead light. The proximity of the light source to the skin allows the use of higher light intensity, which increases the speed of bilirubin breakdown and babies do not need to wear glasses to protect their eyes.
At Evelina London Children’s Hospital we have been using biliblankets to treat neonatal jaundice for more than 10 years. The length of treatment varies and usually lasts from one to five days, however it was noted that infants in two clinical groups required phototherapy for much longer (up to 10 days):
- Premature babies of 34-36 weeks’ gestation. The clearing of bilirubin may take longer in preterm babies and jaundice often reaches the level for treatment on day 3 or 4 of life when the parents have gone through a period of establishing feeding and are tired of being in hospital.
- Term infants with haemolytic jaundice who did not undergo exchange transfusion. Exchange transfusion removes the bilirubin as well as the cause of it. Without exchange transfusion, babies with haemolytic disease continue to produce bilirubin at a higher rate for a period of two to three weeks.
In these babies, the bilirubin level can persistently hover around the treatment threshold level. As per NICE (National Institute for Health and Care Excellence) guidelines,2 treatment should only be stopped once the serum bilirubin level has fallen to at least 50μmol/L below the treatment threshold. The need for phototherapy is the only reason these infants require hospitalisation.
In 2016 a team of neonatologists at Evelina London, including a few enthusiastic paediatric trainees, decided to explore the possibility of delivering phototherapy treatment in the patients’ homes. The team searched the internet for any reports of phototherapy delivered to neonates at home with the hope of learning from the experiences of others and thus avoiding common pitfalls and mistakes. However, nothing was found other than reports of phototherapy use on adult dermatology patients and adverts from private companies encouraging Singaporean parents to purchase bili-blankets for their own babies.
It was decided that we would draft a process where we could use equipment and structures already available at Guy’s and St Thomas’ NHS Foundation Trust without the need for any extra funds or resources. The maternity team was willing to allow the use of its biliblankets as the same patients would have used these if the baby was not transferred home for continuation of the treatment. The neonatal outreach team agreed to provide daily visits with clinical review and blood sampling. The on-call neonatal team would oversee clinical practice and give advice in problematic cases.
A group of parents whose babies were receiving phototherapy on the postnatal ward were surveyed about the idea of delivering the treatment at home. The feedback on the project was overwhel-mingly positive and encouraging, especially from the parents of babies receiving extended treatment (>3 days) who reported a strong desire to be transferred home. Armed with this encouragement, we drafted the process and guidance with a standard operating procedure.
Aims
The aims of the project were to:
- introduce home phototherapy for the management of neonatal jaundice in clinically stable babies
- promote mother-baby bonding and improve the patient/family experience of neonatal jaundice by reducing the length of the hospital stay
- ensure the process is safe.
Eligibility criteria
Infants were considered for home phototherapy if they fulfilled the eligibility criteria:
- The infant had been receiving photo-therapy treatment in hospital for at least 48 hours with stable or falling bilirubin levels. Only babies who could be bled only once in 24 hours could be recruited because of the working hours of the neonatal outreach nurses. At the commencement of phototherapy, more frequent bilirubin monitoring (4-8 hourly) is required. Due to limited availability of staff to frequently monitor bilirubin (which would be necessary should the levels rise), we could only offer this option to babies who we knew had static bilirubin levels or were on a downward trend.
- The infant was likely to require prolonged phototherapy, eg because of prematurity (34-37 weeks’ gestation) or a positive direct antiglobulin test (DAT) confirming haemolytic disease. The average treatment of phototherapy is about 2-4 days but in the two clinical groups we targeted, we very often observed the need for much longer treatment (7-10 days).
- The infant’s weight was not more than 10% below birth weight. All newborn babies are observed to lose some weight after birth; up to 10% of birth weight loss is normal and acceptable. If more weight loss is observed, it may indicate additional health problems.
- Feeds were established (either breast or formula feeding).
- There were no other contraindications to safe discharge (eg the baby was still receiving antibiotics for infection).
- The infant’s address was within the Trust’s catchment area. St Thomas’ Hospital is a local hospital to the population of Lambeth and Southwark and the neonatal outreach team operates within this area. The maternity unit, however, attracts a much wider population such that 50% of women giving birth at St Thomas’ are not local to the Trust (through their choice). We therefore are unable to provide the same service to all women who deliver at St Thomas’.
Enrolment
The steps to enrolment onto the photo-therapy at home pilot study can be seen in FIGURE 1.
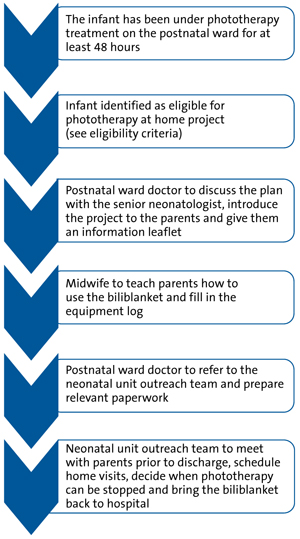
FIGURE 1 The flowchart for enrolment onto the phototherapy at home project.
The equipment
Before leaving the hospital, parents were given an information leaflet (FIGURE 2) and trained to use the fibre optic phototherapy blanket. The baby lies on a blanket that incorporates fibre optic cables; light travels through the fibre optic cables and shines on to the baby’s back. The aim is to expose the baby’s skin to as much light as possible. We use both the biliblanket (the older version of the equipment) and the BiliSoft Phototherapy System (the newer type).
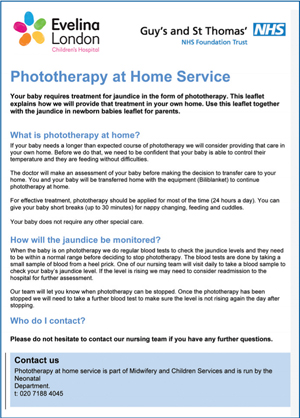
FIGURE 2 The parent information leaflet.
To be able to trace the equipment as property of the hospital, we documented which family was currently using which machine in an equipment log. In time, it turned out to be unnecessary as the neonatal outreach team were supervising the use of the machines and were bringing them back to hospital once the treatment was complete.
Phototherapy at home
There are many different ways that the biliblanket can be used:
- blanket underneath the baby
- blanket over the baby
- in the cot or pram
- during cuddles
- wrapped under the baby during feeding.
Phototherapy should be applied for as much time as possible to speed up the bilirubin breakdown process. Short breaks are allowed (30 minutes every three hours) without detriment to the effect of treatment. The fibre optic source of light is beneficial because it allows continuation of treatment even during feeding. Breast-feeding is encouraged; formula feeding is used through maternal choice or lack of maternal breast milk.
The outreach programme
Once at home the outreach team would visit the family daily, perform feeding and hydration assessments including weight, take a blood sample for serum bilirubin measurement and bring it back to the hospital for testing. Monitoring of bilirubin levels in infants who have received phototherapy needs to be via laboratory measurement and not via a transcutaneous bilirubinometer (the light treatment reduces the level of bilirubin within the skin and so the readings are not considered reliable). When the results are available the outreach staff would plot them on to the NICE phototherapy treatment threshold chart and a manage-ment plan would be made in conjunction with the neonatal doctors.
Each baby would have its own gestational age-specific phototherapy chart on which to plot bilirubin levels. As per NICE guidelines, we would stop phototherapy once serum bilirubin had fallen to a level at least 50μmol/L below the phototherapy threshold and perform another test 24 hours later to check the level was still firmly below the line. In theory we would have to re-admit the baby to hospital if the bilirubin level rose significantly and was within 50μmol/L of the exchange transfusion threshold, which would warrant continuous multiple phototherapy (two sources of light at the same time). In practice, we have never had a case where this was necessary.
The first patient
The first patient was discharged home to continue treatment with phototherapy in May 2017. Mother Zoe Wingfield gave birth to her twin daughters Freya and Megan six weeks early. Although both girls received phototherapy treatment for jaundice at the hospital, Freya required treatment for longer – Zoe and her partner Jon Shaw were the first parents to take home the biliblanket (FIGURE 3). Zoe says: “I had been in hospital for over a week before the girls arrived and then a further week once they were born so it felt like I had been there forever. We couldn’t wait to get home and settle our babies so being able to take them together made a huge difference. The support we received was amazing and we felt confident treating Freya at home because we had used the biliblanket on the ward with Megan.”

FIGURE 3 The first patient to receive phototherapy at home using a biliblanket.
Results
Between May 2017 and May 2018, 10 babies went home for phototherapy as part of this pilot project. Additional babies could have been recruited during this period but only these 10 lived within the pre-defined geographical area.
The characteristics of the infants in the pilot study can be seen in TABLE 1. Two of the 10 babies had a positive DAT and both needed phototherapy for >10 days. No adverse events were noted in the pilot project.
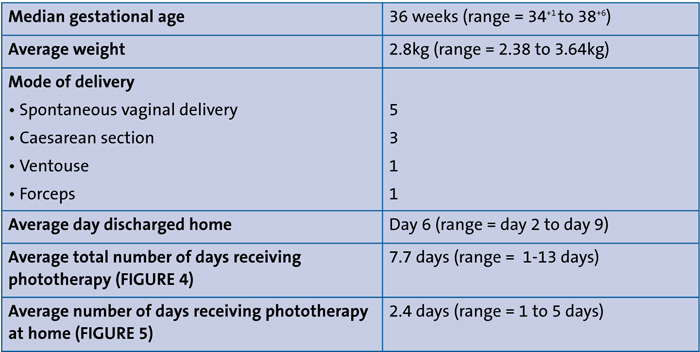
TABLE 1 The characteristics of the 10 babies in the pilot study.
Cost analysis
There are costs associated with a stay of a baby on the postnatal ward and its mother who is a ‘healthy lodger’. On average, women who give birth at St Thomas’ Hospital stay in for 24 hours (ranging from six to 72 hours). In the period of six days, when one baby occupies one cot receiving phototherapy, there could be six other women and babies passing through the postnatal ward.
Prolonged hospital stay on the postnatal ward has an impact on the hospital birth centre, slowing patient flow and leading to, in extreme circumstances, birth centre closures. We estimate the cost to the NHS as a whole is £350 less per baby for home treatment with a biliblanket versus traditional models of care.
Parent feedback
Excellent feedback was received from the parents involved. Some examples include:
“Being on the ward for a lengthy period of time is tough; we couldn’t wait to get home and settle our babies, and this allowed us to do that.”
“The process and equipment worked really well… it couldn’t have worked better for us.”
“I think it is a fantastic idea to allow people to do this, the outreach team that supported us was fantastic.”
“We were desperate to get home and we all really benefited from being at home in our own space.”
Discussion
Within the pilot period 10 babies successfully received phototherapy at home for the management of their neonatal jaundice. It was well received by parents and was safe with no reported adverse events. The neonatal outreach team often commented how pleasant those visits were because of the overwhelming gratitude from parents.
The majority of babies (60%) in the pilot study were born at ≤36 weeks’ gestation. Eight babies (80%) received phototherapy for a total of at least six days. Two of the babies who received the longer (six days or more) total period of phototherapy were DAT positive and four were born at ≤36 weeks’ gestation. Our initial assumption was confirmed: being DAT positive and born at ≤36 weeks are risk factors for needing prolonged phototherapy.
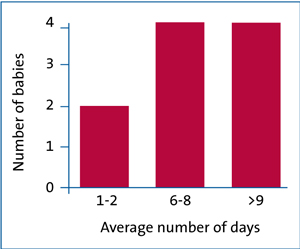
FIGURE 4 Average total number of days that babies received phototherapy.
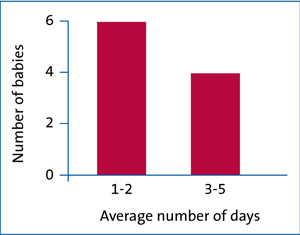
FIGURE 5 Average number of days that babies received phototherapy at home.
Some of the preterm babies ended up receiving their phototherapy at home for only one or two days. After all, there is no way of knowing for certain which of the babies will need prolonged treatment at the time of discharge. There is a balance between trying to discharge babies early for continuation of treatment and assuring no other health issues are at play that may compromise safety.
Neonatal jaundice is the fourth most common reason for a term admission into a neonatal unit and the most common reason for admission from home. NHS Improvement’s Atain (avoiding term admissions into neonatal units) programme advocates activities that may help reduce harm to babies by reducing term admission to the neonatal unit.3 We believe our phototherapy at home prog-ramme is one possible solution, which also reduces hospitalisation of preterm babies.
Since May 2018, phototherapy at home for infants requiring prolonged treatment has become routine management at Evelina London. We continue to discharge about 10 infants a year to complete treatment at home. Overall, the patient characteristics remain the same: preterm or term with haemolytic disease of the newborn. There was, however, one patient with an unclear reason for the need for prolonged phototherapy; the most likely explanation being sepsis. There were also two babies for whom we decided to commence the treatment at home. The two preterm babies (referred from community) were seen daily on the neonatal unit for assessment of jaundice with bilirubin levels close to, but not exceeding, the threshold. Eventually the threshold was met and having had a period of observation and knowledge that their jaundice was rising very slowly, we felt confident that the monitoring of bilirubin levels could continue on a 24-hourly basis.
There is potential to roll this project out to different level 1-3 neonatal units across the UK. As we become more confident in the process babies might be discharged sooner to continue their management at home.
In autumn 2018, one of the junior doctors involved with the analysis of our pilot project moved onto their next placement and learnt that there is another team in London providing phototherapy at home. The Whittington Hospital at Home team (a team of community nurses providing hospital standard care to patients in their homes) has started offering a similar service but using a different model.4 They commence phototherapy treatment at the patient’s home for jaundiced babies who present to the emergency department, in this way avoiding hospital admission of the babies. Both Evelina and Whittington teams have joined forces now to try and promote this new service to the wider community. Applying these two approaches – continuation at home of phototherapy commenced in hospital and commencing new treatment at the patients’ homes – could significantly help to reduce the number of babies needing to stay in hospital. This story also highlights how valuable trainee doctors are in sharing and spreading ideas when they rotate during their specialist training.
During preparation of this publication, we also discovered there are neonatal units in Scotland offering home phototherapy to neonates. This treatment is offered only to term babies and without evidence of haemolytic disease. Our pilot project provides evidence that phototherapy at home can be safely used in preterm infants and in neonates with haemolytic disease of the newborn.
Or read this article in our
Tablet/iPad edition
- Biliblankets are a user-friendly form of phototherapy treatment for hyperbilirubinaemia.
- Home phototherapy reduces the number of babies needing a hospital stay.
- Providing there is appropriate training for parents and support from the outreach team, a home phototherapy programme is feasible, safe and well received by families and staff.
Also published in Infant:
