

Even less invasive: refinement of the LISA procedure improves success with less sedation
The LISA (less invasive surfactant administration) procedure is established as the preferred method for surfactant administration in the neonatal unit at St Peter’s Hospital. A previous audit published in Infant in 2017 detailed our experience with LISA; since then, we have refined the process and this has led to the use of less sedation, improved success rates and maintained comfort for babies. Rescue surfactant is now being administered at lower oxygen thresholds, in line with the local guideline. In this article we describe the changes made and present the results of a re-audit.
Anne W.Y. BehMBChB, MRCPCH, PG Cert HCL
Paediatric ST6
Emily C. Taylor
MBChB
Paediatric ST2
Peter R. Reynolds
MB.BS, MSc, PhD
Consultant Neonatologist
peter.reynolds1@nhs.net
@neonataldoc
NICU, Ashford and St Peter’s Hospital NHS Foundation Trust, Chertsey
Local refinement of LISA
Over the past two years there has been a gradual increase in interest from the UK neonatal community in the LISA procedure – the administration of surfactant directly into the trachea via a fine tube or catheter. Meta-analyses published in 2016 demonstrated reduced risks of bronchopulmonary dysplasia (BPD) and death, where surfactant is administered via the LISA approach compared to conventional administration via an endotracheal tube.1,2 More recently, a large observational study from Langhammer and colleagues reported the outcomes of two matched groups of 148 very low birthweight infants born in the German Neonatal Network. The numbers of babies receiving subsequent mechanical ventilation in the LISA group was significantly reduced (34% vs 86%) and they received fewer analgesics and sedatives too.3
Since we published the results of an audit of LISA in Infant in 2017,4 our practice has significantly changed, which has led to a refined and even less invasive approach. In this article we describe the changes and the results of a re-audit.
Approach
In the previous audit, we reported that the four key elements for a successful procedure were: correct timing of LISA; pre-procedure preparation; use of ‘awake’ sedation; and training and supervision. We have made changes in these areas based on small plan-do-study-act (PDSA) cycles, which has enabled us to make rapid changes based on practice evaluations.
Timing of LISA
We continue with our aim to give rescue surfactant when we believe that there is significant respiratory distress syndrome (RDS). This is most often based on clinical judgement accompanied by evidence of a rising fraction of inspired oxygen (FiO2) despite delivery of nasal high flow at flow rates of 7-8L/min. However, that clinical judgement can also be exercised in the delivery room as well as on the neonatal intensive care unit (NICU) therefore we have equipment for LISA ready on our resuscitation trolley. We still use a threshold of FiO2=30% (regardless of gestation), but aim to also consider:
- the rate of rise of FiO2
- the work of breathing (which can be difficult to objectively assess)
- evidence of impaired lung function (eg increasing transcutaneous carbon dioxide levels)
- risk factors for RDS (eg prematurity, antenatal steroids, the likelihood of sepsis, an infant of a mother with diabetes)
- factors that might affect oxygen requirement, such as ensuring establishment of adequate lung expansion (eg ensuring adequate nasal high flow rates) or general handling.
A chest X-ray is not mandatory to diagnose RDS and we are exploring the role of lung ultrasound.
Preparation
This has now changed substantially since our previous audit. The introduction of the LISAcath (Chiesi), a catheter for oral endotracheal instillation (FIGURE 1), has considerably simplified the procedure. We increasingly try to use videolaryngoscopy in our routine clinical practice although we find that new users need to adjust their techniques, especially to ensure a full view of the cords before attempting the procedure, and that equipment is not always available.

FIGURE 1 LISAcath – a catheter for oral endotracheal instillation of surfactant.
Safety checks, the continued application of non-invasive ventilation (as nasal high flow), and planned avoidance of hypo-thermia remain important. Likewise, it remains important for our teams to recognise that this is still a delicate and critical care procedure and they need to be ready to escalate their airway/respiratory management if the baby deteriorates.
Use of awake sedation
We have largely discontinued the routine use of sedation, which is another significant change. This has been primarily enabled by the procedure now being much less invasive than it previously was. The elimination of the need for Magill forceps and the introduction of videolaryngoscopy, means that first time laryngoscopy is enhanced and is quicker. Once the LISAcath is in place, the laryngoscope is removed and, for the vast majority of babies, the ‘worst’ of the procedure is swiftly over. As a result, we no longer routinely administer sedation (in the form of fentanyl), but this can be used if required. Premedication with atropine is also optional and is used at clinical discretion too, although now far less commonly. Importantly we aim to ensure that the baby is settled and comfortable. There is an emphasis on swaddling, and using oral sucrose even in the smallest babies is encouraged. The tolerability of the procedure was a key part of the audit.
Training and supervision
The use of a videolaryngoscope has vastly enhanced training/simulation and also the ability to supervise a safe procedure. It has given staff the opportunity to see the procedure in real time. Videolaryngoscopy also enables the creation of videos for training purposes (FIGURE 2). There remain ongoing concerns about the confidence and competence of doctors and advanced neonatal nurse practitioners (ANNP) in training to visualise the cords and introduce a catheter. In our view, the advantages of videolaryngoscopy are significant but there is a need for structured and supervised training. As we only use one system (Storz, C-MAC) we are not able to compare different videolaryngoscopes and consider that this would be a useful exercise.
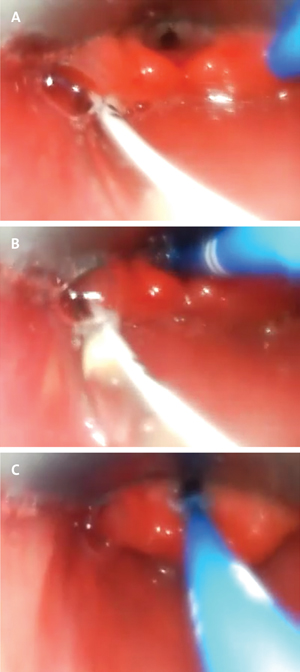
FIGURE 2 Images from videolaryngoscope footage showing placement of the LISAcath. (A) View of the vocal cords with advancement of the blue LISAcath. (B) LISAcath inserted to 1.5cm below the vocal cords. (C) Midline position of LISAcath with white surfactant visible just above the catheter.
Audit
A proforma for collection of audit data was designed (FIGURE 3) and this was completed post-procedure by the clinician who performed the technique. Audit data were collected over a six-month period on 36 different infants who underwent the LISA procedure (n=40). In four babies, LISA was repeated at a different attempt. Three attempts in a single procedure were permitted, otherwise the procedure was deemed to have failed. Need for immediate intubation was also deemed a failure of LISA.
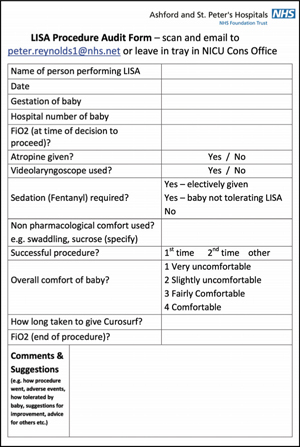
FIGURE 3 The proforma for the collection of audit data.
The median gestation was 29+1 weeks (range = 24+4 to 37+0) and the median time from birth to LISA was 18 hours (range = 2 to 91 hours). The median FiO2 when LISA was commenced was 35% (range = 29 to 75%), which fell to 24% (range = 21 to 70%) by the end of the procedure. Only two infants required immediate intubation at the time of LISA for failing to respond (5%) and notably they both had very high FiO2 at the time LISA was attempted (≥60%). Of the remainder, only 7.9% (n=3) were intubated within 24 hours of LISA. The median duration for admin-istration of surfactant was five minutes.
Babies were assessed on a simple four-point scale (very uncomfortable/slightly uncomfortable/fairly comfortable/ comfortable) by the nursing staff who were assisting with the procedure. The audit results showed that comfort scores were lowest in the more mature population. For procedures rated as very uncomfortable or uncomfortable the median gestation was 33+1 weeks, whereas for babies rated as fairly comfortable or comfortable the median gestation was 28+2 weeks, which was a significant difference (p<0.01). There were no differences in comfort, gestation, or the grade of the operator associated with the success of LISA at the first attempt. Overall the success rate for LISA was 95%. LISA was successful the first time in 55%; in those the videolaryngoscope was used in 64% and non-pharmacological pain relief (either swaddling, sucrose or both) was used in 91%. Importantly, 95% of babies with a successful LISA did not receive sedation. An interesting observation emerged that babies who ‘sucked’ on the laryngoscope blade or catheter were more likely to be given sedation or have a less straightforward procedure.
LISA procedures were carried out mainly by trained junior neonatal medical staff:
- ST4-8 or associate specialist: n=19
- ST1-3 or ANNP: n=20
- consultant: n=1.
LISA was performed at a median FiO2 of 34%.
Discussion
In our experience, the introduction of the LISAcath has made the procedure even less invasive, enhancing the success rates and comfort for staff and baby alike.
We are now achieving a higher success rate for LISA (95%) than in our previous audit (87%). This is despite having changed to the non-routine use of sedation and with a higher proportion of junior doctors performing LISA (97% vs 72%). For the latter, we recognise that there may have been some pre-procedure selection bias.
The substantial reduction in the use of sedation has therefore not resulted in more LISA failures, nor did it lead to concerns that the procedure was very uncomfortable for the majority of babies. In babies where comfort was a concern, the gestation was usually higher. In an audit of 38 babies receiving propofol sedation for LISA, Dekker showed that while the comfort scores were significantly improved in babies who received sedation, they were significantly more likely to require non-invasive positive pressure ventilation during the procedure (100% vs 33%). There was also a tendency for bradycardias to be more prolonged (three vs one minute) and for more babies to require intubation during (9% vs 0%) or within 24 hours of LISA (26% vs 13%).5 These important and undesirable events indicate that we need to be careful to ensure that the benefits of sedation are not outweighed by the potential for harm. The adverse effects of anaesthetic drugs on the preterm brain/organs are largely unknown. None of the babies who were intubated within 24 hours in this audit had received sedation.
We have improved our compliance with our FiO2 target and are now administering surfactant at a median FiO2 of 34%, compared to 45% in the previous audit. We think that this is partly because we no longer have to spend considerable time preparing medications for sedation. There is usually a fall in the oxygen requirement post-procedure, which occurs quickly, however further reductions can occur over the next few hours and this should be borne in mind when considering repeat dosing.
The time from birth to giving surfactant varies considerably and is different to practices in some other countries where surfactant is given much earlier. While rescue surfactant is used over prophylaxis-based on a (rather old) Cochrane analysis,6 it must be remembered that LISA may mitigate the disadvantages of prophylaxis and in the most immature babies it may be appropriate to give surfactant at even lower thresholds. More evidence is needed.
Further work is also needed to establish whether improvements in non-pharmacological pain relief, such as the use of sucrose or breast milk applied to the tongue, would mitigate the need for further administration of sedation/ analgesia, or if there is a population of babies who should routinely receive sedation. Whether this is based on gestation, wakefulness or failure of procedures, for example, is not yet clear. In babies of, ≤32 weeks’ gestation, we think that the procedure should be achievable in the majority of cases without the use of sedation. However, in the rarer event of procedural failure then sedation might improve success rates. Oral ‘responsiveness’ (such as sucking) may not be a reliable indicator but was commented on by some operators as making the procedure more difficult.
The LISA procedure fits well within our non-invasive respiratory strategy at St Peter’s Hospital. We note, however, that LISA is a procedure with significant potential for adverse events. The LISAcath tip is not particularly soft, and operators must have a clear view of the vocal cords and not force or repetitively jab the catheter to achieve placement. We strongly advocate for the use of videolaryngoscopy for supervision and learning. Audits of practice, such as this one, are also very useful for governance and assurance purposes. A recent UK survey showed that LISA was used regularly in under 20% of neonatal units with variations in thresh-olds, sedation and practices.7 National guidelines for the use of LISA are being prepared by an expert working group to support colleagues who wish to introduce LISA into their neonatal practice.
Summary
We have refined and re-audited our LISA guideline. As a result, we have been able to significantly reduce our use of sedation and enable the majority of procedures to be carried out by junior medical staff with an increase in the proportion successfully achieved. We have improved compliance with our aim to perform LISA for RDS where the FiO2 has reached 30% or more. LISA is an integral and routine part of non-invasive lung care at St Peter’s Hospital NICU.
Or read this article in our
Tablet/iPad edition
- Refinements to the LISA procedure have led to improved success rates and a reduction in the use of sedation.
- The majority of LISA procedures are now performed by junior doctors with an increase in those successfully achieved.
- Compliance with our aim to perform LISA for respiratory distress syndrome where the FiO2 is ≥30% has improved.
