

The changing picture of neonatal abstinence syndrome: ‘new drugs on the block’
Neonatal abstinence syndrome (NAS) is usually associated with maternal opioid use but the pattern of drug use is changing, with many affected infants now having been exposed to new psychoactive substances in utero. This article will focus on emerging recreational substances, particularly synthetic cannabinoids, the challenges faced in the management of NAS in these cases, and the potential long-term consequences.
Rachel TooneMBChB, MRCPCH,
PGCertNeonatal Grid Trainee
Kathryn Johnson
MBChB, FRCPCH,
Consultant Neonatologist
Cath Harrison
BMedSci, BM, BS, DTM&H,FRCPCH
Consultant Neonatologist
catherine.harrison10@nhs.net
Leeds Teaching Hospitals NHS Trust
Substance misuse is increasing in all populations but mainly in younger women leading to an increase in the incidence of NAS.1 The term NAS is most often used in the context of maternal opioid use but the pattern of drug use is changing, with many fetuses now being exposed to novel substances, often in the context of polysubstance use. The US Food and Drug Administration has propose the term neonatal opioid withdrawal syndrome, but as polysubstance misuse becomes more common, the more generic NAS term will continue to be used clinically.2
Psychoactive substances
New psychoactive substances (NPS) is now the accepted term for what used to be called ‘legal highs’. Imported mainly from Asia, NPS became increasingly prevalent in the UK from around 2008-2009. Despite the Psychoactive Substances Act in 2016, which banned the production, supply and importation of any psychoactive substances for human consumption, their use has continued to increase.3 NPS are divided into five groups:
- stimulants (similar in effect to cocaine)
- downers (similar to benzodiazepines)
- hallucinogens (similar to LSD)
- dissociatives (similar to ketamine)
- synthetic cannabinoids.
Synthetic cannabinoids are probably the most widely available of these substances and as a result there is greater literature on their potential effects although the effects of the different product groups are not distinct, particularly in the context of polydrug use.
Synthetic cannabinoids are manufactured to mimic the action of tetrahydrocannabinol (THC), the principal psychoactive constituent of cannabis, which acts on cannabis receptors in the brain. This leads to altered perception and feelings of relaxation but also vomiting, seizures, tachycardia, hallucinations and paranoia. THCs are often much more potent than cannabis – up to 660 times so – leading to stronger effects and even death.4
There are over 200 different compounds sold as synthetic cannabinoids in the UK. They are usually consumed either as ‘herbal’ preparations to be smoked, or liquid to be used in e-cigarettes.5 ‘Spice’ is a commonly used term or brand name for synthetic cannabinoids but can refer to a multitude of different chemicals. The contents of these substances can vary widely, even between packets of the same brand. In addition, drugs marketed as synthetic cannabinoids may not actually contain any.6
Antenatal use
Use of NPS is rising in the UK, particularly in the homeless population and prison settings with an association with polydrug use and chaotic lifestyles.7 This is probably due to its relative low cost and easy availability. The 2017-18 Crime Survey for England and Wales reported that 0.8% of females aged between 16 and 24 admitted using NPS in the last year.7 Being a household survey, this is likely to be an underestimate of use, as the homeless and prison populations will not have been included.
In our region (Yorkshire), the use of Spice is rising – a similar picture to other cities in the north of England, with multiple reports of its use in national newspapers. This general increase is reflected in our antenatal population, particularly in women with known polydrug use, chaotic lifestyles and homelessness.
Clinical signs
The classical symptoms of NAS have been well described in the literature (FIGURE 1) but, in the main, these are seen in opioid withdrawal.8 Withdrawal signs or direct effects on the newborn babies of NPS users are not well described, however they have the potential to cause complex prolonged symptoms, particularly as many users of NPS will be polysubstance users.
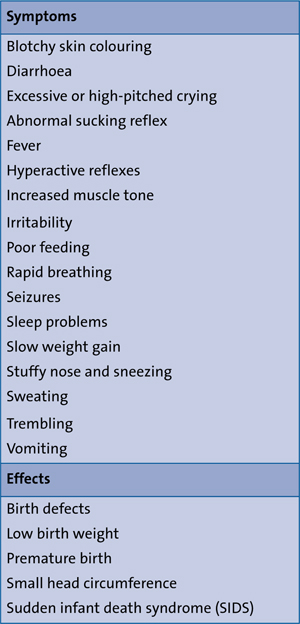
FIGURE 1 Classical symptoms and potentialeffects of NAS. The classical symptoms of NAShave been described for opioid withdrawal. The effects of NPS are not well described and have the potential to cause complexprolonged symptoms.
Management of NAS
Due to the likelihood of polydrug use in this population, routine pharmacological therapy and supportive measures should be tried initially on the understanding that NPS effects in the newborn may be resistant to standard therapy.9 A description of non-pharmacological measures used in the management of NAS is presented in the article by Kumar and Garg in this same issue of Infant.10
Morphine is the most commonly used medication to treat symptoms; it works on opioid receptors. There is variation on how it is used in terms of dosage and weaning. Methadone also works on opioid receptors and is the mainstay of opioid replacement therapy (ORT) in mothers during pregnancy due to its long action and oral preparation. Evidence is emerging to show that methadone may be better in babies compared to morphine, with a shorter length of treatment and thus length of stay.11
Buprenorphine is frequently used as an ORT in pregnant women but can also be used for the treatment of NAS. It has a long half-life, which allows once-a-day dosing. The BBORN trial compared sublingual buprenorphine to oral morphine in 63 infants and found that the babies in the buprenorphine group had a significantly shorter median length of treatment (15 vs 28 days) and a reduction in their length of stay (21 vs 33 days).12 There are, however, some safety concerns about buprenorphine with animal data showing that prenatal exposure to bupren-orphine decreases neurogenesis.12 There are no long-term human studies as yet.
Clonidine blocks the release of noradrenaline and can be added to other treatments, such as morphine, in cases of resistant opioid withdrawal. Although small numbers, studies have shown an improvement in withdrawal symptoms in terms of length of stay and duration of treatment.13
Phenobarbitone is often used for the treatment of non-opioid NAS. Most use it as an adjunct to an opioid due to the likelihood of polydrug use. A Cochrane review showed that infants treated with both an opiate and phenobarbitone had a shortened hospital stay, lower withdrawal scores and needed less opiates.14 Pheno-barbitone has a sedative effect that may be more beneficial in babies exposed to polydrug use.
There is mixed opinion about when to add adjunctive treatments – some suggest when the maximal opioid dose has been reached. Others start combined treatment early when withdrawal scores are rising rapidly suggesting severe withdrawal.
Long-term implications
There is increasing concern about potential behavioural abnormalities caused by a rise in maternal cannabis use.
The endocannabinoid system (ECS) is a biological system composed of endo-cannabinoids, which are neuro-transmitters, cannabinoid receptors, and cannabinoid receptor proteins that are expressed throughout the central nervous system. The ECS system is known to regulate physiological processes such as fertility, pregnancy, fetal and infant development.15-17
Cannabinoids cross the placenta and are secreted in milk during lactation prolonging exposure.18,19 There is accumulating evidence that when exogenous cannabinoids are used, there is an association with impaired embryological development, ectopic pregnancy, miscarriage, low birth weight and premature birth.20,21 There is specific concern about the effects of exocannabinoids on neuronal migration in early pregnancy and animal models have shown teratogenic changes in the nervous system.22 Similar patterns of hyperactivity and cognitive/learning disabilities including memory problems have been shown in both animal models and humans.23,24
There is growing interest in the effects of maternal cannabinoid exposure on the emotional development of children. This is partly because cannabinoid receptors are expressed in brain areas such as the hippocampus, which modulate anxiety, but also because cannabinoids affect the release of other chemicals such as serotonin and dopamine, which are known to influence anxiety.24,25 Knowing this, it could be postulated that maternal cannabis exposure might cause long-term emotional problems in children. Gray describes increased levels of self-reported anxiety and depressive symptoms in 10-year-old children who were exposed to maternal cannabis use.26 However, long-term clinical data are not available.
It is known that timing and duration of exposure can lead to a variation in neurofunctional effects, both in animal models and in humans.27,28 It is difficult, however, to establish the effects from individual drugs in humans due to potential simultaneous exposure to multiple drugs, difficulties in documenting the pattern of use, impact of social or genetic factors, and the challenges in carrying out long-term studies in this population.28
Summary
The prevalence of drug use is rising in our society, as are drug-related deaths and admissions. Healthcare professionals need to be aware of the ‘new drugs on the block’ and the increase in use of these substances, as well as how to manage withdrawal from them and the potential long-term consequence to exposed infants.
Or read this article in our
Tablet/iPad edition
- The pattern of NAS is changing because polysubstance misuse is common.
- Neonatal healthcare professionals need to be aware of new drugs, how to manage withdrawal from them and the long-term consequences to exposed infants.
- Medications used for management of NAS include morphine, methadone, buprenorphine, clonidine and phenobarbitone.
