

Parent-led ward rounds on the neonatal unit
Feedback from parents shows that they want to be involved in all aspects of their baby’s care, with the support of healthcare staff. Where ward rounds are concerned, this is usually taken to mean parental presence, or perhaps ‘taking part’ in ward rounds by being able to ask questions at the end. However, parents are ideally placed to lead the ward round – not just observe. They are the constant throughout their baby’s stay, and have only their own baby (or babies) to focus on.
Oliver RackhamNeonatal Consultant, Glan Clwyd Hospital, Betsi Cadwaladr University Health Board, North Wales (formerly Arrowe Park Hospital, Wirral University Teaching Hospitals NHS Trust) oliver.rackham@wales.nhs.uk
Family-integrated care is a model of care that incorporates the family into the neonatal team as partners caring for their baby. This has been shown to improve outcomes for the baby and family, and also prepare the parents for the transition from hospital to home. Feedback from parents shows that they want to be involved in all aspects of their baby’s care, with the support of healthcare staff. Where ward rounds are concerned, this is usually taken to mean parental presence, or perhaps ‘taking part’ in ward rounds by being able to ask questions at the end.
Parents are ideally placed to lead the ward round – not just observe. They are the constant throughout their baby’s stay, and have only their own baby (or babies) to focus on.
Ward rounds
Feelings are always mixed on how to best conduct ward rounds. One key question is whether the parents of other babies should stay in the room. In a spacious unit it is easier to maintain confidentiality when other parents are present but with less space between cots this can be difficult and some units may decide to ask other parents to leave so that sensitive or emotional topics can be discussed in a confidential manner.
The neonatal intensive care unit (NICU) at Arrowe Park Hospital provides care for babies born from 23 weeks’ gestation. The unit strives to be supportive to parents, enabling them to gain confidence in caring for their baby.
While having an open visiting policy, practice at Arrowe Park is to ask parents to leave when other babies are being discussed. This was decided after surveying parents on their preferences. In Glan Clwyd Hospital’s sub-regional NICU, with more space between cots, all parents are able to stay in the room during ward rounds. Some units have instituted different measures, eg headphones with music for the other parents.
Prior to the introduction of parent-led ward rounds at Arrowe Park, parents consistently fed back to us that hearing a list of problems every day was distressing, particularly when many were no longer applicable. They also told us that it could be scary hearing about progress in clinical terms, especially in the earlier part of the stay. When the health professionals spoke, parents said they felt left out and on the outside. When they were asked if they had any questions, they felt ‘a bit thick’ asking for explanations of medical terms. They did, however, value the ward round and the opportunity to hear directly from doctors.
Feedback from parents was used as a driver for change; we decided upon a format to trial after discussion and suggestions from some of the graduate parents.

Parents presenting their baby at ward round in Glan Clwyd Hospital.
Introducing parent-led ward rounds
No real preparation was needed to start running the parent-led ward round – we just needed to tell the parents, doctors and nurses what to expect. We did not alter the timing or pattern of the ward rounds. The parents continued to stay for their own baby but were asked to step outside while we discussed other babies.
We gave out information sheets to parents a few days in advance, which explained what it would mean, and the introduction said:
Hello, we would really like to give you the opportunity to present your baby on the ward round this week. This just means saying how old they are, what they weigh now, how they are doing with feeding, etc. If you don’t want to, or don’t feel able to, don’t worry; we’ll just carry on as normal and you can tell us or ask us anything at any time.
We made it clear that this was entirely voluntary and parents could participate as much or as little as they wanted. We stressed that it was not a test and we would work out all the information between us. We gave them a brief outline to the kind of things we would normally talk about and we supplied pens and paper in case they wanted to make any notes. For example:
- name
- gestation at birth, number of days old today (corrected age)
- birth weight and weight now
- the main issues at the moment:
- breathing support or help
- feeding
- medicines
- head scans
- eye screening
- immunisations, etc
- plans for the next day or two
- plans towards discharge
- planned discharge date.
Conducting parent-led ward rounds
As long as we give them the opportunity, all parents will lead a ward round in a way that suits them. We wait for the parents to be there before starting. We address the opening questions to them – open ended, so that they can say as much or as little as they want. We ask how they are and then how their baby is.
We don’t ask the nurses and doctors anything until the parents have said or asked all they want to. This means we get their key messages and also address the things that matter most to them. This changes throughout the stay and even on a day-to-day basis.
Some parents do not want to start the discussion and are happy to chip in with comments and information. Others will wait until the end and then ask their questions.
Some parents will just say something along the lines of: “she’s fine,” “he’s been OK on CPAP overnight,” “his feeds were stopped again,” “we’ve taken his tube out.” Others want to give a bit more information about progress, changes or the questions they would like answering. Often it evolves from “she’s OK” into a fairly comprehensive discussion as they expand on what matters to them.
Parents are generally not ready to present their baby in the first few days of an intensive care admission, but will still let us know what is important to them. Once a baby has been in the unit for a while the parents are more likely to present. Most do this by discussing key changes in the past 24 hours, usually relating to respiratory support or feeding. If the ward round starts in this way and the doctor or nurse presents other aspects of information, parents are more likely to contribute. They are also more likely to make suggestions regarding care when we start the ward round with them.
Some parents present their baby in a structured way, either with written notes or from memory. There are many reasons that they are perfectly placed to do this; as the parents spend time in a neonatal unit they become experts in the terminology and jargon. They know their own baby’s journey in great detail and do not have to worry about mixing up information between patients. They remember dates (due date, date of extubation, retinopathy screening, immunisations, etc) without needing to look them up. They remember when and in what order events happened.
What are the benefits?
Parents feel that they are a part of the team. Including them as fully as possible fosters a strong relationship between the parent and child as well as with the healthcare team.
This makes open and honest discussions more likely. Parents are more likely to speak to us, the healthcare professionals, about con-cerns they may have as well as the questions they would like to ask.
Parents presenting offers a great opportunity to check that their understanding of the situation is the same as that of the doctors and nurses. An example was of feedback from a parent who was told that ‘the bleed on the brain is stable’ when they hadn’t been notified of it in the first place. It is too easy to assume that we have told parents things when we have not, or that they have been able to take in the information and understand it at the time when we did tell them. If that parent had been leading the ward rounds, this would not have happened.
Parents had told us that what was most important to them was often not discussed, eg a likely discharge date. This is an important topic from very early on for some parents – it gives them hope and if we do not let parents lead the discussion we may not fulfil their needs.
Feedback
Feedback has been good, with parents appreciating the opportunity to be an integral part of the team (FIGURE 1). Parents commented that they need to present their child when they attend GP, emergency department, assessment ward or clinic appointments and so it was very useful to be doing that in the neonatal unit.
Some staff were wary at first, fearing that this would be taking something away from them. However, once they realised that it only adds to the content of the ward round, this fear seemed to resolve.
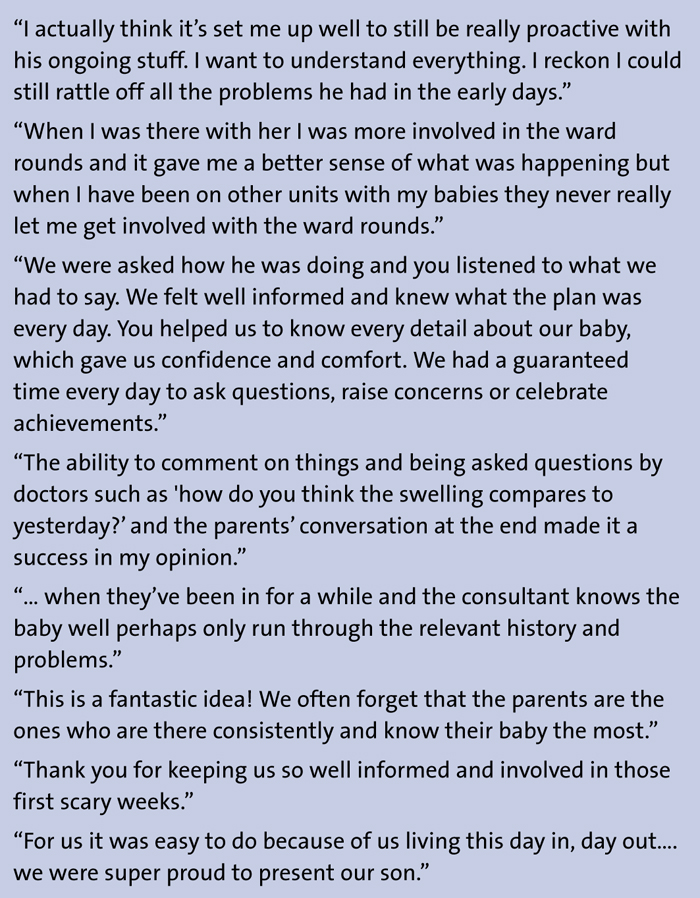
FIGURE 1 Parent-led ward rounds: parent feedback.
What problems did we encounter?
Parent-led ward rounds are not for everyone and it must be made clear to staff and parents that it is voluntary and that we are happy to carry on as normal if the parents do not want to lead. Some parents simply will not want to; others may feel unable to do this at all or perhaps not until they are making plans for home. Some parents may feel this is a negative experience – they may feel under pressure to do it, or made to feel inadequate for not. It is important for staff not to coerce and to look out for signs of any distress in the parents. If staff do not pick up on this, some parents may even avoid ward rounds.
It is possible that, while addressing issues key to the parents, the staff could miss or forget to address other important issues. However, the staff will still have all of the information in the patient record, and the parent-led ward round does not replace the structured assessment of the baby and recording of that assessment by the healthcare team. We did receive some concerns that discussions between doctors and nurses could become limited; although this might relate more to the parents’ presence on ward round rather than whether or not they present their baby. If the parents’ presentation is simply added on to the ward round, then there is a risk that the ward round may become too long. It is important that staff use the information from the parents in the same way as that from the staff themselves. This problem is not limited to parent-led ward rounds and can be seen when information shared during handovers and safety huddles is repeated during a ward round.
If parents are not present at the time of ward round a decision has to be made whether to continue without them. This will depend on where they are in their neonatal journey and what they have expressed as important to them. The parents need to know the details beforehand, eg what time they will be seen, what order the ward round might take, how much they will be involved in the discussion. It is important to ensure that this information is communicated to them.
Many babies are transferred between units for acuity of care needs or for capacity reasons. A difference in practice between units can often confuse parents, and their level of input on the ward round may also be different as they move between units. This can cause distress and needs to be discussed with the parents of a baby who is likely to move between units. This is an area of concern for many other aspects of care (such as nasogastric tube feeding, preparing and giving medicines, taking and recording temperature, etc) and so should not be a barrier to implementing parent-led ward rounds. In North Wales we are rolling out a formalised family-integrated care package across the three neonatal units. This will include information about parent-led ward rounds and will hopefully alleviate some of these differences.
Arrowe Park is a smaller NICU where one consultant is responsible for all babies each week. This does lend itself well to parent-led ward rounds. However, there is no reason that larger or even surgical units could not run parent-led ward rounds for the ‘main’ round(s) of the day. If space is limited and other babies’ parents are not able to stay during ward round, there may be logistical problems regarding timing – this is more relevant to the discussion of parents being present on ward rounds than to whether the parents present their baby.
The use of video
We were lucky to have some parents who were happy to be filmed presenting on ward round. This has enabled us to demonstrate how easy it is to carry out successful parent-led ward rounds and their value. We use the video for teaching health professionals to improve their interactions with parents and staff. Filming the different styles of parent presentations could be useful for staff education and reflection.
With consent we have shared two videos of parents presenting on Twitter:
1. https://twitter.com/OliverRackham/status/1048247824222175234?s=19
2. https://twitter.com/OliverRackham/status/1117854264049557504?s=19
These were very well received with some excellent comments as well as some questions and challenges. We found this to be a great way of spreading the idea of parent-led ward rounds and receiving valuable feedback. We have had lots of questions from staff in other units and have shared our experience with them. Some asked whether information that the parents do not have direct access to (eg blood results) might be missed. Reassuringly, the staff who normally conduct ward rounds are still present with any notes, observation charts, results, etc and they can provide that information either when the parents mention it or after the parents have finished speaking. We also received some helpful feedback about the placement of computers during ward rounds as they can impede communication, and also regarding parents sitting while staff stand. These are general ward round challenges but we have been able to adjust practice to take these kind of comments into account.
Or read this article in our
Tablet/iPad edition
