

Airway management in neonatal intensive care units: the PIC-NIC survey
Improvements in airway management have occurred in almost all UK adult intensive care units following the publication of the Fourth National Audit Project (NAP4) in 2011. Subsequently the PIC-NIC survey investigated whether the lessons learned from NAP4 had filtered into paediatric practice. This article highlights the relevant findings for neonatal healthcare professionals by discussing the high-risk nature of neonatal airway management and strategies that might be used to improve safety including planning for difficulty, immediate access to emergency airway equipment and the role of continuous waveform capnography and videolaryngoscopy.
Katie E. FoyClinical Fellow
Timothy M. Cook
Consultant, Department of Anaesthesia and Intensive Care Medicine
Bernie Marden
Consultant in Paediatrics and Neonatology
Fiona E. Kelly
Consultant, Department of Anaesthesia and Intensive Care Medicine
Royal United Hospitals Bath NHS Foundation Trust
Management of the neonate who requires intubation and ventilation can be associated with many risks, including failure to intubate the trachea and unrecognised intubation of the oesophagus. Both situations, if not rapidly identified and managed, can lead to hypoxia, hypoxic brain injury, poor neurological function and in some cases bradycardia, cardiac arrest and death. Once intubated, the neonate who is dependent on a tracheal tube remains at risk of complications including tracheal tube displacement and obstruction.
NAP4 was carried out by the Royal College of Anaesthetists and the Difficult Airway Society and recorded all major complications of airway management in the UK within a one-year period.1 Reported cases were analysed for common themes and lessons. NAP4, published in 2011, was a landmark study, with one key finding being that airway management in intensive care units (ICUs) is very high risk, with an airway complication resulting in death or brain injury being around 60 times more likely than in the operating theatre.1 NAP4 identified that lack of planning for difficulty, lack of immediate access to emergency airway equipment, inadequate airway training for ICU staff and a lack of continuous waveform capnography contributed to poor outcomes in intensive care. The failure to use continuous waveform capnography, or incorrect interpretation of capnography waveforms, was reported to contribute to >70% of the ICU deaths reported.1
Two years after NAP4, 80% of UK adult ICUs reported changes in practice in response to NAP42 and it is highly likely that the safety of airway management has been improved as a consequence. In 2013, continuous waveform capnography was always or often used in 97% of UK adult ICUs for intubation and in 89% for monitoring of a patient who was depen-dent on a tracheal tube. Continuous waveform capnography is now mandated in UK and European ICU guidelines.3-5
The scientific literature suggests that neonatal airway management is also a high risk area. Adverse events follow 22-46% of neonatal intubations6,7 and severe desaturation (defined as >20% from baseline saturations) occurs in 51% of intubations.6 Oesophageal intubation is the most common complication,6,7 and first-attempt success at intubation is only 64% for experienced neonatologists, dropping to 20-22% for more junior members of staff.8
It is likely that sharing of best practice between ICUs in different parts of the hospital can be very advantageous. There is certainly much that adult ICUs can learn from neonatal ICUs (NICUs), including presence of parents on ward rounds, involvement of clinical psychologists, extensive follow-up clinics and regional retrieval teams.9 The PIC-NIC survey was carried out to investigate whether the lessons learned from NAP4 had filtered into PICU (paediatric intensive care unit) and NICU practice.9 This article focuses on the neonatal findings of the PIC-NIC survey.
The PIC-NIC survey: methods and results
A telephone survey of all UK NICUs was conducted by speaking to a member of senior nursing staff or a doctor of registrar grade or above. Local neonatal units and NICUs were included in the survey (all referred to here as NICUs); 143 units were identified and a complete response was received from 129 units (90%).9
The survey comprised 19 questions and was carried out between January and October 2016. The key findings of the survey are summarised in TABLES 1 and 2. A similar survey was carried out among UK PICUs and the results are included for comparison. Full methodology and results can be seen in the original Anaesthesia paper.9
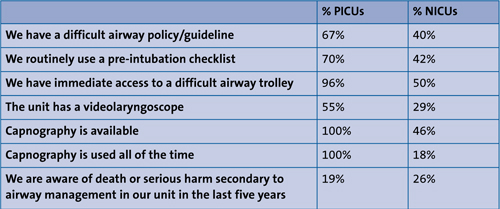
TABLE 1 A summary of key findings from the PIC-NIC survey, which looked at airway management in PICUs and NICUs.
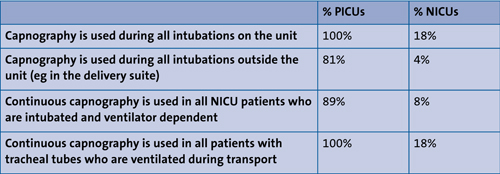
TABLE 2 The PIC-NIC survey: findings pertaining to capnography.
Discussion and implications for neonatal practice
Following the publication of the PIC-NIC survey, there has been much discussion in the scientific literature10-13 and on social media. Much of this focused on capnography, but it is important to note that the survey had other equally important findings. While airway training is provided by 97% of NICUs,9 the use of intubation checklists, an immediately available difficult airway trolley in the NICU, protocols for management of the difficult neonatal airway and inclusion of patients with difficult airways at NICU handovers might be inexpensive means of improving patient safety (TABLE 1). These strategies are all standard practice in adult ICUs.
The use of continuous waveform capnography in the NICU to both confirm the correct placement of a tracheal tube at intubation and to continuously monitor that the tracheal tube is patent and in the correct place during mechanical ventilation has proved controversial: some NICUs and neonatal transport teams are using this monitoring for all patients all the time, while other NICUs judge that it is not technically possible.10-14
The role of videolaryngoscopy (using a laryngoscope with a camera on the blade, which relays a picture of the larynx onto a screen) in neonates is still unclear,15 but the evidence base and enthusiasm for video-laryngoscopy in adult practice over the last five years suggests that this could be a growth area in NICUs. In adult practice, videolaryngoscopes have been shown to enhance the view at laryngoscopy, reduce difficult and failed intubations, and improve training, team work, communication and human factors.16
Conclusion
In summary, the PIC-NIC survey reported wide variation in neonatal intensive care practice and identified some areas that may deserve further investigation and discussion among NICU clinicians. Some adult ICU airway strategies may be transferable to NICU practice. The use of continuous waveform capnography for both confirmation of intubation and airway monitoring during mechanical ventilation may warrant discussion. The British Association of Perinatal Medicine framework for practice for clinical management of the difficult airway in the perinatal period, currently in progress, is likely to shine a light on this important area and the authors hope that it will examine routine airway management as well as difficult airway management.
Conflict of interest
The Royal United Hospital Department of Anaesthesia has been loaned or received airway equipment at cost price or on loan for evaluation, research and teaching.
Timothy Cook has visited several airway companies to talk or offer advice, without payment.
Or read this article in our
Tablet/iPad edition
- Airway management in intensive care units (ICUs) is high-risk and contributes to morbidity and mortality in the neonatal unit.
- The PIC-NIC survey reported wide variation in practice between NICUs.
- Adult ICUs have much to learn from NICUs; similarly, NICUs can learn much from adult ICUs. Some areas of best practice may be transferable to neonatal settings.
