

The Great North Neonatal Biobank: using salvaged samples to facilitate novel translational research in preterm infants
Translational research in preterm infants is key to their future health but there are many challenges associated with this type of research in this population. This article describes the establishment of the Great North Neonatal Biobank (GNNB), along with the research facilitated to date. The future opportunities that GNNB and other biobanks may offer are explored.
Janet Elizabeth Berrington
MB BS, MD,
Consultant Neonatal Paediatrician and Honorary Senior Lecturer
Newcastle Neonatal Service, Newcastle upon Tyne Hospitals NHS Foundation Trust and Newcastle University
j.e.berrington@ncl.ac.uk
Amy Peasland
BSc (Hons), MSc, PhD
Biobank Manager, Newcastle University
amy.peasland@newcastle.ac.uk
Research improves care and outcomes for trial participants by a variety of mechanisms1 but research in preterm infants, especially that which requires biological samples, is challenging both ethically and practically and particularly difficult in the tiniest and most immature babies. These babies have the highest rates of ‘preterm-associated diseases’ such as necrotising enterocolitis (NEC) and late onset sepsis (LOS), and biological specimens are not easy to obtain, particu-larly at or around the onset of disease. Yet potentially they are the samples researchers need most – samples that will allow them to begin to unlock the mechanisms associated with preterm specific diseases, where animal models are limited and no paediatric or adult equivalent disease exists.
Taking biological samples purely for research is, quite rightly, restricted. A 500g baby has a circulating blood volume of just 40mL. Although specifics of guidance around sampling for research varies by country and institute, we cannot take more than 3-5% of the total blood volume (1.2-2mL for a 500g baby) and not more than 1-5% on any single occasion (0.4-2mL),2 which severely restricts studying very preterm infants either longitudinally or frequently around a key event such as NEC.
To address this, a study was designed to improve mechanistic understanding of NEC and LOS in preterm (<32 weeks’ gestation) infants based on a salvage system where ‘waste’ specimens could be utilised (with parental permission). This was the SERVIS study (supporting enhanced research in vulnerable infants), which was reported soon after it commenced3 and included permissions to utilise residual SERVIS samples in other ethically approved work. These waste specimens included:
- any residual blood left after routine testing (including ‘one-spot’ dried blood spots that were not needed)
- stool, urine, breast milk and other routinely suctioned fluids such as oral or nasal secretions
- biopsy or surgically resected tissue in excess of that needed for diagnostic requirements, as well as access to formalin-fixed paraffin embedded tissue once reporting was complete.
These samples are particularly valuable as they are linked to a large amount of demographic, exposure and outcome data collectively described by the term ‘deeply phenotyped’, the most useful attribute that biobank samples can hold.4
The SERVIS study permitted the specific predetermined analyses included in the SERVIS protocol, which resulted in inc-reased understanding of NEC and LOS.5-12 This, along with the recent explosion in ‘omics’ capacities, the large number of samples that were acquired and did not get used quickly, and the potential to use these with newer technologies (at Newcastle or by other research groups), led to the development of the GNNB (FIGURE 1).

FIGURE 1 Staff at the GNNB, Newcastle University.
Purpose and aims of GNNB
The GNNB set out to formalise the existing collection of specimens into a sustainable biobank with capacity to add to this from:
- infants already contributing as they age
- newly born infants.
The aims of GNNB are summarised in FIGURE 2 with the overall objective being to support research that promotes survival without impairment and the long-term health of babies born preterm, small or sick.
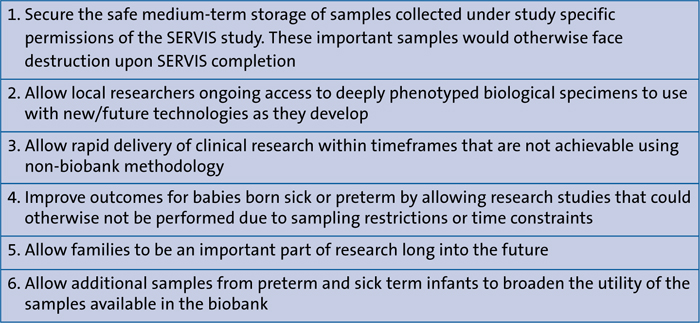
FIGURE 2 Aims of the GNNB.
Routes to biobanking specimens
Infants can contribute specimens through one of two mechanisms:
- separate biobank consent where the intent is to deposit all samples into the biobank
- via a consented neonatal study that also includes consent for residual samples to move to the GNNB.
These other ethically approved studies are generally in the preterm population, and they may be intervention studies, however no interventions are administered to patients as part of the biobanking process. Contributing studies include the mechanistic study MAGPIE (mechanisms affecting the preterm gut in enteral feeding trials),13 which is embedded into the large UK trial of lactoferrin to prevent late onset sepsis (ELFIN).14
Biobank specific consents are used for infants >32 weeks’ gestation who therefore are not eligible for SERVIS (but may, for example, have a congenital anomaly requiring gut surgery providing tissue that can be banked).
Non-invasive samples from healthy term infants can also be obtained under the biobank consent processes (eg urine, stool, breast milk and saliva) and these are used for control experimental purposes. Consents are obtained for each type of biological specimen and these can be selectively declined if desired. They include consent for work outside the UK or by commercial companies and animal work, with appropriate constraints around profit use and, again, each of these can be selectively declined.
Existing collaborators of the Newcastle neonatal team in the UK and abroad can deposit samples in the GNNB, which are collected and processed as previously described, subject to local modifications while maintaining ‘link anonymity’. Material transfer agreements exist for transfer between sites. Researchers with similar suitable samples but with whom no existing collaboration exists can deposit samples in GNNB upon application and for an appropriate fee.
Samples
Samples stored in the GNNB are surplus to diagnostic requirements and only collected at the time of necessary clinical procedures with the exception of urine and stool, which are collected deliberately and non-invasively from the nappy.
An established system is used, which informs laboratory technicians of permissions relating to blood samples from infants on the ward and successfully retrieves residual specimens where permissions exist. Where tissue removal occurs as part of clinical need (most commonly bowel resection for NEC) surplus specimens can be banked. Post-mortem specimens (where parents give consent on the standard post-mortem consent form for use in research) are also available to researchers through GNNB mechanisms but are not physically relocated until specific research is undertaken on them.
Anonymisation procedures
All samples are stored link anonymised. Immediately after collection and clinical use (where relevant) all identifiable details are removed. Samples are then identified using a unique biobank number and dated (FIGURE 3). Biobank records refer to these numbers only.

FIGURE 3 Sample labelling for the GNNB. All samples are stored link anonymised and are identified using a unique biobank number.
Clinical data
Biobank codes are linked to detailed clinical data held about each newborn baby in a secure database, extracted from patient records and existing electronic databases. This includes demographic data, clinical diagnoses, clinical management/ therapeutics and outcomes. Consent is specifically sought on the consent form for access to this data for research purposes. Access to the clinical dataset is limited to the chief investigator. Any data released to investigators of specific approved projects are released linked to the biobank code only.
Permissions for translational research
GNNB permissions allow for samples to be analysed and used in a wide range of translational techniques, dependent on both the sample type and current local projects. This includes, but is not limited to those in FIGURE 4. The protocol also acknowledges the rapid developments in this field and does not limit use to those techniques currently listed.
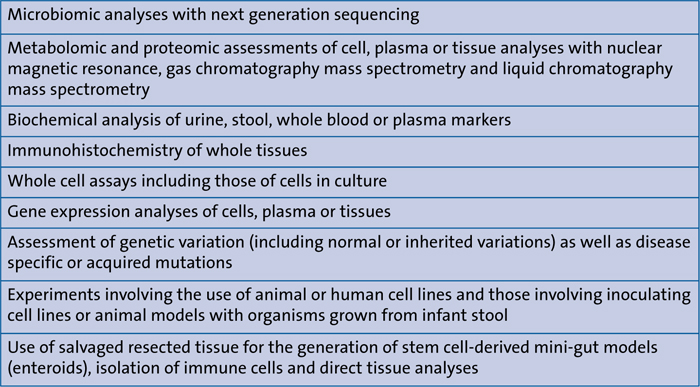
FIGURE 4 Current permissions relating to translational research capacity.
Funding arrangements
Tiny Lives, a local neonatal charity, has supported the initial projected costs, estimated to cover the first three years of the GNNB with a £15,000 grant. Ongoing grant applications where GNNB samples will be used, or where GNNB is a repository for samples collected in new studies, include in their funding bids an amount designed to maintain biobank viability.
Ethical approval and governance
The GNNB holds full ethical and local approvals; the designated individual is that for Newcastle University Human Tissue Authority (licence number 12534). The approvals prevent the need for future local studies using samples in the GNNB to seek separate ethics approvals.
Non-Newcastle studies seeking to access GNNB specimens do require separate ethics approval when an application for access to specimens is made, and must be made using a specific form.
A GNNB access and governance committee assesses these requests with additional representation from Tiny Lives and clinical neonatologists. This committee ensures that any project requesting use of the samples is scientifically sound, a worthwhile use of specimens, and has adequate funding and appropriate ethical approval.
The principal investigator (PI) of the approved project must submit a brief report to the governance committee on completion of the study and is encouraged to acknowledge GNNB in any associated publications. The PI must cooperate with audit requests made by the tissue bank governance committee (eg around sample tracking).
Reporting
An annual report is submitted to the Newcastle University ethics committee and Newcastle Hospitals NHS Foundation Trust Research and Development including:
- number of each sample type collected
- summary information of all applications made to the biobank along with the protocols of successful applications
- reports from completed studies
- number of tissue samples released
- number of tissue samples returned for replacement in the biobank
- summary of currently held samples.
Feedback
Parents are key to the success of the GNNB and were integral to its establishment. Information about research studies that have used GNNB samples is published on our publicly accessible website (www.neonatalresearch.net) and a link to this is provided for parents in the information leaflet. Feedback from parents has been sought and this has been universally positive. Comments through website feedback and Facebook include:
- “Anything that speeds up research for parents and babies has got to be good.”
- “It’s a great idea… and gets my backing.”
Research findings are reported in the scientific literature and presented at national and international scientific meetings. These will also be reported back to families.
Research facilitated to date
In addition to the SERVIS studies, five infants of >32 weeks’ gestation have been recruited in the two years since the GNNB received full permissions. This has provided fresh gut samples for successful development of mini-gut models (enteroids) and facilitated research with external groups using salvaged blood samples for a study into genetic susceptibility of NEC and infection, and stool samples for exploration of preterm gut health (publications for which will follow).
Future opportunities
Using the GNNB for research has the significant advantage that samples are already collected from a group of otherwise hard to sample patients where disease occurrence (or health) is already known. Samples from infants experiencing rare events can be provided much faster than if these infants and samples had to be recruited and collected prospectively. This is especially important where illnesses are rare and sporadic, as in the case of NEC. These processes can hasten study results and make research much cheaper to conduct. The authors wish to encourage researchers who could use GNNB samples to contact them by email.
Conclusions
Translational research is especially challenging in the neonatal period. The salvaging biobank facilitates rapid delivery of neonatal research, particularly for diseases that are specific to preterm infants or neonates and where learning cannot be transferred from older infants. Such systems deserve financial and practical support.
Or read this article in our
Tablet/iPad edition
- Research improves care and outcomes for preterm infants but biological sampling specifically for research purposes is practically and ethically challenging and limited by patient size.
- A ‘salvage’ system was established for a specific research study. To avoid disposal of these valuable specimens, a biobank was created for these and other samples for use in future research.
- The aims and process, parental perspectives, challenges and successes are described to promote the use and development of other similar collections
Also published in Infant:
