

The red hat pathway: reducing avoidable NNU admissions for hypoglycaemia
Although untreated neonatal hypoglycaemia may be a cause of long-term harm, anticipatory management of at-risk babies (eg with thermoregulation and feeding support) can prevent many unnecessary admissions. Staff at the NNU at Evelina London Children’s Hospital implemented the ‘red hat pathway’ to reduce the number of avoidable NNU admissions for hypoglycaemia by introducing the use of a red knitted hat for babies identified as at increased risk. The project demonstrates that many of these at-risk infants can be successfully managed on the postnatal ward and highlights how a simple intervention can have a significant impact on care delivery.
Jennifer McGrath
Senior Clinical Fellow in Neonatology
Joy Simmonds
Paediatric Trainee
Natasha Stephenson
Paediatric Trainee
Grenville Fox
Consultant Neonatologist
Malgorzata Radomska
Neonatal Associate Specialist
Neonatal Unit, Evelina London Children’s Hospital
jennifer.mcgrath1@gstt.nhs.uk
The Atain (avoiding term admissions into neonatal units) programme identified hypoglycaemia as a leading cause of term admissions to neonatal units (NNU) and set out to reduce the number of full-term infants (>37 weeks’ gestation) admitted.1 Although untreated neonatal hypoglycaemia may be a cause of long-term harm, anticipatory management of at-risk babies (eg with thermoregulation and feeding support) can prevent many unnecessary admissions. Many babies who do not have clinically significant hypoglycaemia could be cared for on the postnatal ward, which keeps the mother and her baby together.1
Inspired by Atain, staff at the NNU at Evelina London Children’s Hospital implemented the ‘red hat pathway’ via a plan-do-study-act (PDSA) cycle to reduce the number of avoidable NNU admissions for hypoglycaemia. Prior to implementation, a retrospective audit of NNU admissions of babies at risk of hypoglycaemia was performed, which looked at admission data for February to April 2017 using the UK Maternity and Neonatal Patient Data Management System (BadgerNet). Those at risk were defined as:
- infants of diabetic mothers
- infants born 34-37 weeks’ gestation
- growth restricted infants or infants with a birth weight below the second centile.
Cold stress may be associated with hypoglycemia in the newborn and interestingly over half of these babies were noted as cold on admission.
The red hat pathway
In addition to the existing local hypoglycaemia practice guideline, we set out to introduce the use of a red knitted hat for babies identified as at increased risk of hypoglycaemia. Before rolling out the new pathway on 1 August 2017, we asked a large group of local volunteer knitters if they could provide these hats. We produced information leaflets about hypoglycaemia in the newborn for parents, and for staff we prepared a standard operating procedure and education and awareness campaigns (FIGURE 1). We attended maternity ‘huddles’ to speak to the midwives and healthcare professionals on the postnatal wards. Staff update sessions were provided in order to highlight the new pathway before it was rolled out.

FIGURE 1 The red hat poster, aimed at raising awareness of the project among staff.
The red hat pathway is essentially the same as the existing hypoglycaemia pathway, the only difference being that a knitted red hat is worn and an information leaflet is given to the parents. At handover the red hat babies are highlighted to identify their heightened care requirements. Also they are identified to the doctors on the postnatal ward as babies that still need to receive daily reviews. The red hat is worn for a minimum of 24 hours until temperature and blood sugars have stabilised, or for 12 hours after blood sugar monitoring has stopped because blood sugars have stabilised.
PDSA
In February 2018 we collected some interim audit data that indicated there were fewer babies being admitted to the NNU for hypoglycaemia and fewer with hypothermia. We also surveyed parents and staff at the birth centre and postnatal ward to canvas opinion. The survey results showed:
- very positive feedback regarding the project as a whole
- the midwives felt the red hats were very helpful in handover
- the postnatal ward midwives expressed concern that babies often came to the ward without their red hats
- the leaflets were not routinely handed out with the hats
- the leaflets may have too much information and be overwhelming for parents
- there is no consistent way to document if a baby is/has been a red hat baby.
In summary the midwives expressed that it was really helpful to visibly label these babies although there was some inconsistent use of the red hats and information leaflets on the postnatal wards and at the birth centre.
At this point we ran more awareness sessions to ensure that everyone was familiar with the pathway. We also made sure we had plenty of red hats and that these were co-located with the parent information leaflets so that they could be handed out together as a bundle.
A retrospective re-audit of NNU admissions was performed 11 months after implementation in May 2018 and the data pre- and post-pathway introduction were analysed using statistical methods (chi-square test and/or Fisher’s exact test).
Results
Introduction of the red hat pathway significantly reduced the NNU admission rate for babies with hypoglycaemia from 15 babies per 1,000 live births to 6.8 (TABLE 1).
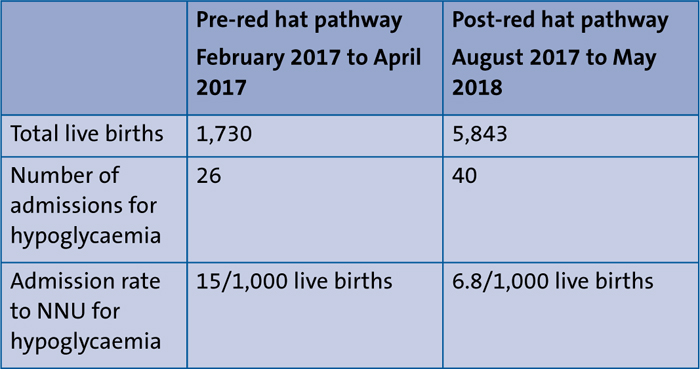
TABLE 1 Reduction in admission rate per 1,000 live births for hypoglycaemia.
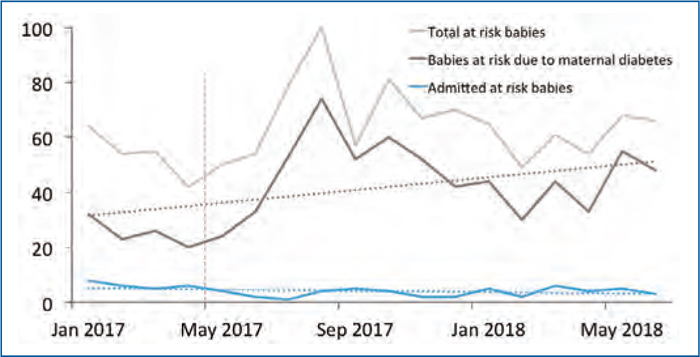
In May 2017 the obstetricians and midwives implemented a new gestational diabetes mellitus (GDM) screening programme (FIGURE 2). Following this, there was increased identification of mothers with GDM and a greater number of at-risk babies. Despite this, the risk of admission for hypoglycaemia for at-risk babies was significantly reduced (TABLE 2) and if a baby was admitted, there was a significantly reduced risk of it being hypothermic and hypoglycaemic (TABLE 2).
FIGURE 2 Babies admitted to the NNU over time. Note, the number of at-risk babies increased from May 2017 because of the introduction of a new screening guideline for GDM (red vertical line). Despite this, at-risk babies admitted to NNU remained reasonably stable. The majority of our at-risk babies come from mothers with diabetes, hence babies at risk due to maternal diabetes closely follow total at-risk babies.
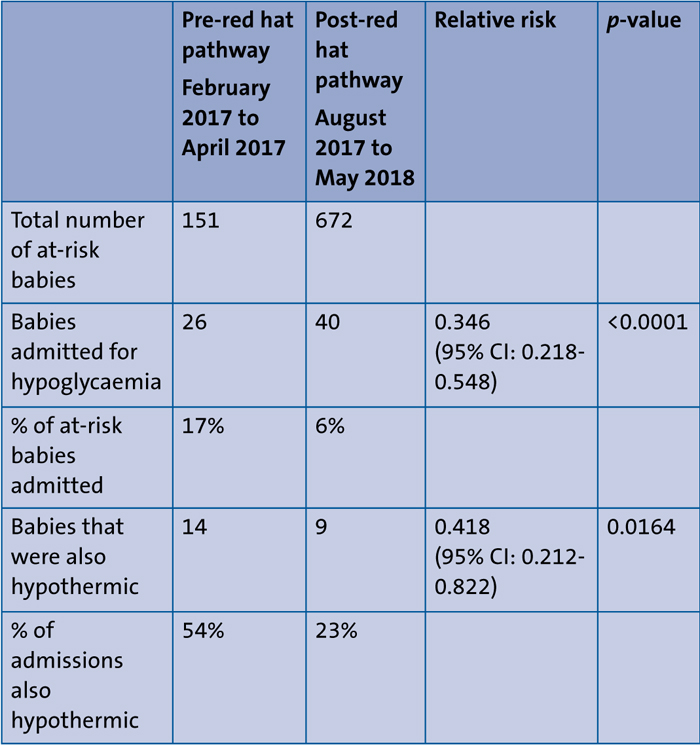
TABLE 2 The risk of admission for hypoglycaemia for at-risk babies was significantly reduced, as was the risk of a baby being hypothermic when admitted with hypoglycaemia.
These results suggest that many of these at-risk infants can be successfully managed on the postnatal ward with high quality care and good awareness among midwives and parents of their care needs. This project highlights how very simple interventions and strong teamwork between specialties can have a significant impact on care delivery.

A red knitted hat identifies babies as at-risk for hypoglycaemia.
Future directions
One hurdle, as a consequence of a fully paperless system, was the lack of a means to record red hat babies on BadgerNet. To address this, a red hat tick box is in the pipeline for introduction.
Mothers with diabetes will have at-risk babies, therefore the diabetes midwives have started to hand out the parent information leaflet to these mothers at their 36-week appointments.
In line with most other units, a new hypoglycaemia guideline based on the British Association of Perinatal Medicine (BAPM) Framework for Practice2 was introduced at the end of May 2018. Our new guideline fully incorporates the red hat pathway as routine practice; a re-audit is planned to ensure ongoing compliance with the pathway and to assess the combined impact of these two interventions.
Acknowledgement
With thanks to Zeshan Rawn, Information Manager at Evelina London Neonatal Unit, for his help with accessing the data and Manisha Choudhary (Paediatric Trainee), Omer Homida (Paediatric Trainee) and Dareilena Karaviti (Junior Clinical Fellow in Neonatology) for their help with the project. Special thanks to all of the midwives, parents and babies for their support and involvement.
Or read this article in our
Tablet/iPad edition
