

BAPM’s latest framework for practice: Q&A
The British Association of Perinatal Medicine (BAPM) has launched a new framework for practice: Optimal arrangements for local neonatal units and special care units in the UK including guidance on their staffing. This framework provides guidance on optimal activity levels and additional guidance on medical staffing for local neonatal units (LNUs) and special care units (SCUs) in the UK.
Wendy Tyler
Consultant Neonatologist, Shrewsbury and Telford NHS Trust
Grenville Fox
Consultant Neonatologist, Evelina London Children’s Healthcare
Steve Jones
Consultant Neonatologist, Royal United Hospital, Bath
Alan Fenton
Consultant Neonatologist, Royal Victoria Infirmary, Newcastle
Why was this framework for practice needed?
Operational delivery networks (ODNs) are now well established in the UK as a means of providing care for newborn infants. Neonatal units within each ODN are designated as SCUs, LNUs and neonatal intensive care units (NICUs). While cot capacity is a key component of effective ODN function, medical and nursing staffing and activity are equally important and have been less well described. In 2014 BAPM authored a framework for practice describing optimal activity and medical staffing in NICUs.1 Given the large proportion of neonatal care undertaken outside of NICUs, it seemed appropriate to develop an aligned framework for SCUs and LNUs to support the delivery of safe, high quality care.
How was the framework developed?
BAPM surveyed all UK LNUs and SCUs from mid-2016 through to early 2017 for staffing information. Activity data for three years (2013-15) were shared directly from BadgerNet with the per-mission of the network leads.
What was measured?
Respiratory care days (RCDs) and admission weight were chosen to reflect activity, as research informed the use of RCDs and birth weight <1.5kg within the NICU framework. Comparable evidence-based data for LNUs and SCUs are currently unavailable although the ongoing OPTI-PREM study (optimising neonatal service prov-ision for preterm babies, 27-31 weeks) may address this for LNUs.
RCDs are defined as all days during which a patient received invasive or non-invasive respiratory support; it excludes days in which oxygen is administered via low-flow nasal cannulae or head box or directly into an incubator. Admission weight <1.5kg is defined as the weight on admission to the unit including from birth or a later repatriation. Mean values were calculated for both RCDs and admission weights. Where units closed or merged during this time, the mean was calculated for the number of years that they were providing care.
What was found?
The number of RCDs delivered correlated with the number of babies admitted to units with an admission weight of <1.5kg (FIGURE 1). But:
- There was wide variation in the number of RCDs delivered between units admitting the same number of small babies. Extreme examples are the two units admitting around 86 babies annually where the RCDs delivered are 1,000 and almost 3,000 (circled in FIGURE 1; the reasons for this variation were outside the scope of the framework).
- LNUs and SCUs are, in general, separate in their activity levels, although there is some overlap. The activity data within the framework support the observation that the two types of unit are distinct.
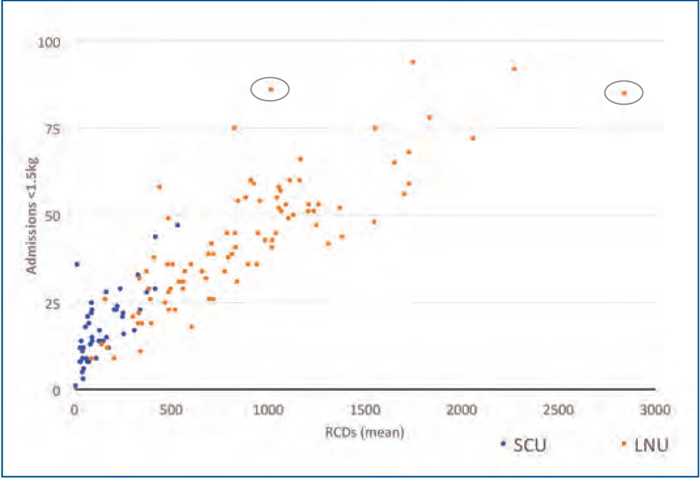
FIGURE 1 The number of RCDs delivered correlated with the number of babies admitted to units with an admission weight of <1.5kg, however, there was wide variation in the number of RCDs delivered between units admitting the same number of small babies. The two units admitting around 86 babies annually (circled) are an extreme example.
So what about staffing?
Many LNUs did not achieve Toolkit for High Quality Neonatal Services2 staffing standards, which require all LNUs to have a dedicated tier 1 staff member 24/7 separate from paediatrics. This ensures that they are immediately available to the neonatal unit and labour ward. Just over half of LNUs complied with this recommendation (FIGURE 2, in green). The two units in blue had completely shared staffing with paediatrics at all times, with the remaining units (in orange) having partially separate staffing – an example would be shared staffing for some or all of out-of-hours, including weekends.
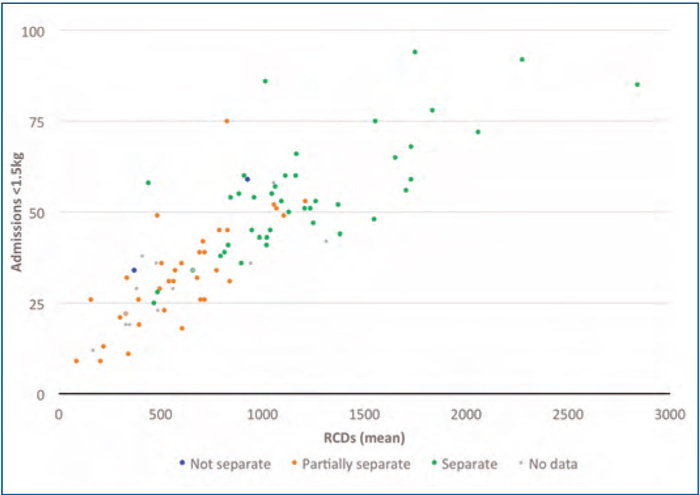
FIGURE 2 Tier 1 staffing availability (LNUs).
LNU tier 2 and 3 staffing also varied: just over one-fifth of LNUs had separate dedicated tier 2 staffing while nearly one third had separate consultant staffing from paediatrics 24/7. In general, the larger activity units had separate tier 3 staffing, presumably a requirement to ensure that senior staff could be available for both paediatrics and neonatology in these larger busier units, particularly if the tier 2 was shared out-of-hours.
Why weren’t birth rates or intensive (IC) and high dependency (HD) care days used instead?
Available birth rate data could not be substantiated and sources such as MBRRACE-UK present their information by trusts, a number of which contain several neonatal units with merged birth rate and outcome data.
So what does it all mean?
Recommendations: activity
- Units designated as LNUs should admit ≥25 infants <1.5kg admission weight and perform 365 RCDs annually
- SCUs should anticipate admitting up to 25 infants <1.5kg admission weight or undertake up to 365 RCDs annually.
There are a number of LNUs with activity levels in 2013-15 below those recommended. Double the number of LNUs would have had sub-optimal activity levels if a definition of ≥500 RCDs was chosen. Given the potential impact on babies, families, staffing and transport services within the UK, the working group defined LNU minimal activity as 365 RCDs as a consensus opinion currently pending further research. Of note, 365 RCDs is equivalent to 500 combined IC+HD days (FIGURE 3).
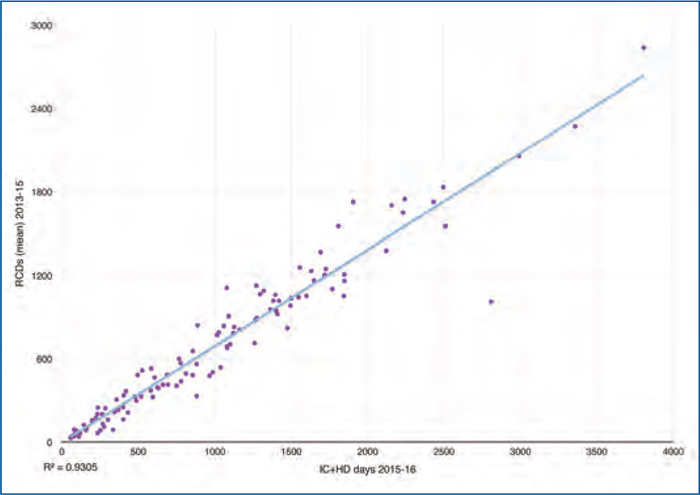
FIGURE 3 England LNU + SCU RCDs (mean) 2013-15 calendar years vs IC-HD days 2015-16 financial year.
IC days (England Clinical Reference Group) correlated with RCDs: a strong correlation between combined IC+HD days and RCDs for LNU+SCU in England was found (FIGURE 3).
There are SCUs with activity levels above those recommended and ODNs should ensure enhanced staffing levels are available even when redesignation is not viable, to support safety and quality of care.
Recommendations: staffing
The tables provide the detail of the staffing recommendations for differing levels of activity within LNUs (TABLE 1) and SCUs (TABLE 2). The green boxes show the activity levels at which separate dedicated tier staffing is recommended while the gold boxes show the activity levels at which, if separate dedicated 24/7 staffing is not available, a risk analysis should be performed and the results shared and acted upon. This should include placing the risk on the trust’s risk register with escalation to trust board as per local arrangements, and sharing with the ODN.
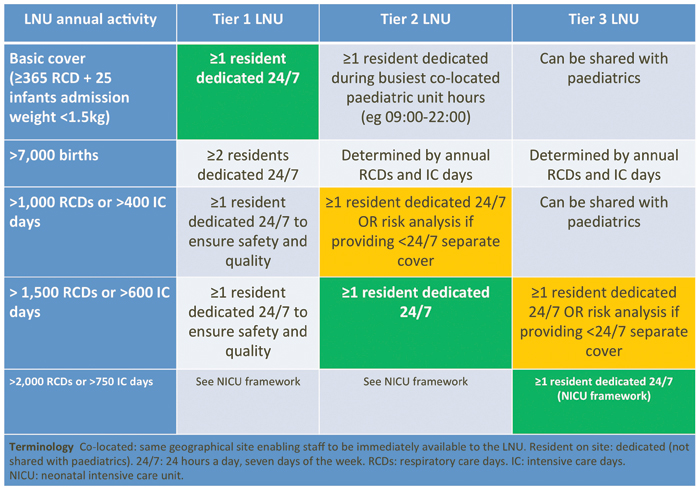
TABLE 1 Staffing recommendations for LNUs.
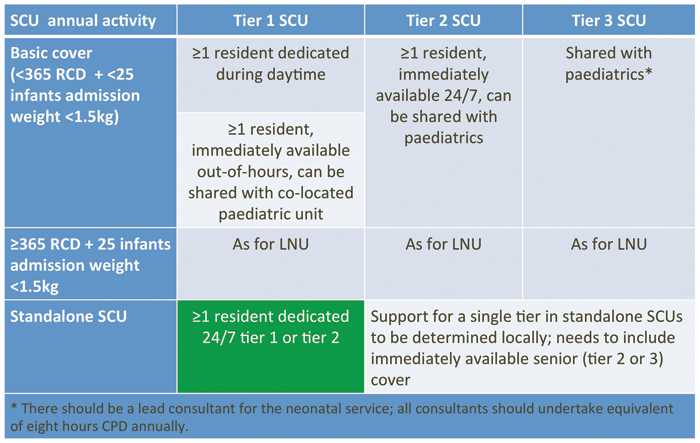
TABLE 2 Staffing recommendations for SCUs
So what happens next?
Links with national neonatal service reviews
Scotland has launched its neonatal service review3 and England has shared the detail of its recommendations, most recently as part of the NHS Long Term Plan.4 The BAPM framework seeks to support these national reviews by reinforcing and expanding the 2009 Toolkit staffing level recommendations and defining the current minimum activity levels expected of our units delivering newborns of ≥27 weeks’ gestation.
The Neonatal Critical Care Transformation Review (NHS England) recommends that LNUs will provide care for all babies born at their hospital of ≥27 weeks’ gestation, >800g birth weight or multiple pregnancies ≥28 weeks’ gestation. This includes short-term IC where necessary, with LNUs receiving babies of 27-31 weeks’ gestation requiring HD care from SCUs as transfers. The review also recommends that SCUs should provide local care for babies born ≥32 weeks’ gestation and >1,000g birth weight, who require only special care or short-term HD care.
A minimum LNU activity level of 1,000 IC/HD days per year is, recommended in the Neonatal Critical Care Transformation Review in order to facilitate safe and sustainable staffing levels in the future. This level is equivalent to around 750 RCDs (FIGURE 3) and has implications for a significant number of current LNUs. This recommendation would require significant local recon-figuration and therefore a five-year timescale has been suggested.
Results from the OPTI-PREM trial and further research for LNUs and SCUs should be used in future to determine relationships between activity, staffing and outcomes for both types of unit to ensure recommendations are based on quality outcomes and safety.
Where can I find out more?
The document Optimal arrangements for local neonatal units and special care units in the UK including guidance on their staffing: a framework for practice was published by the BAPM working group in November 2018 following a period of consultation over the summer. The framework and the responses to the consultation can be found together at: www.bapm.org/LNUSCU
Summary
- There is a lack of evidence underpinning activity and staffing in LNUs and SCUs.
- There is currently wide variation in activity and admissions in LNUs and SCUs.
- The BAPM Framework for LNUs and SCUs seeks to provide guidance around medical staffing, activity levels and numbers of admissions of babies <1.5kg.
Acknowledgment
The authors would like to thank all the neonatal teams that responded to the LNU SCU BAPM survey, the LNU SCU working group who contributed to the framework development, and the ODN leads (in particular Martyn Boyd) for distributing the survey.
Or read this article in our
Tablet/iPad edition
