

MBRRACE-UK Perinatal Mortality Surveillance Report: UK perinatal deaths for births in 2016
The fourth MBRRACE-UK Perinatal Mortality Surveillance Report presents information on extended perinatal deaths in the UK and Crown Dependencies arising from births during 2016. This report continues MBRRACE UK’s work to collect, analyse and report national surveillance data in order to stimulate and evaluate improvements in health care for mothers and babies.
Elizabeth S. Draper
Professor of Perinatal and Paediatric Epidemiology, University of Leicester on behalf of the MBRRACE-UK perinatal surveillance team and collaborators
In June this year we published the fourth MBRRACE-UK Perinatal Mortality Surveillance Report where we present information on extended perinatal deaths in the UK and Crown Dependencies arising from births during 2016. This report continues our work to collect, analyse and report national surveillance data in order to stimulate and evaluate improvements in health care for mothers and babies. The report focuses on the surveillance of all late fetal losses (22+0 to 23+6 weeks of gestational age), stillbirths, and neonatal deaths for births in 2016, with data presented by country, by geographical area, healthcare provider (trusts and health boards) and local authority.
As in previous reports the main findings are presented in a combination of maps and tables showing both the crude and the stabilised and adjusted mortality rates for stillbirths, neonatal deaths, and extended perinatal deaths (stillbirths and neonatal deaths combined). Stabilisation is designed to take account of some of the random variation inherent in these types of data and adjustment takes account of some of the factors known to affect perinatal mortality rates in particular populations, eg the level of social deprivation.
In order to ensure comparability of mortality rates, data are shown after excluding births occurring at less than 24+0 weeks of gestational age and terminations of pregnancy. However in addition, this year’s report also contains, for the first time, national gestation-specific numbers and mortality rates for babies born at 22+0 to 23+6 weeks of gestational age.
The full report is available on the MBRRACE-UK website with the report infographic, summary report and slide sets. These are free to download from www.npeu.ox.ac.uk/mbrrace-uk reports. Here we present a few of the key findings from this latest report.
Mortality rates
MBRRACE-UK has collected data for four years across the whole of the UK (a cohort of well over two million births) and has seen a year-on-year improvement in the quality of the submitted data. This has allowed us to explore time trends in extended perinatal mortality, stillbirth and neonatal mortality rates for the UK. In 2016 the extended perinatal mortality rate for the UK was 5.64 per 1,000 total births, a reduction from 6.04 per 1,000 total births in 2013. This represents approximately 300 fewer baby deaths in 2016 compared with 2013 (FIGURE 1).
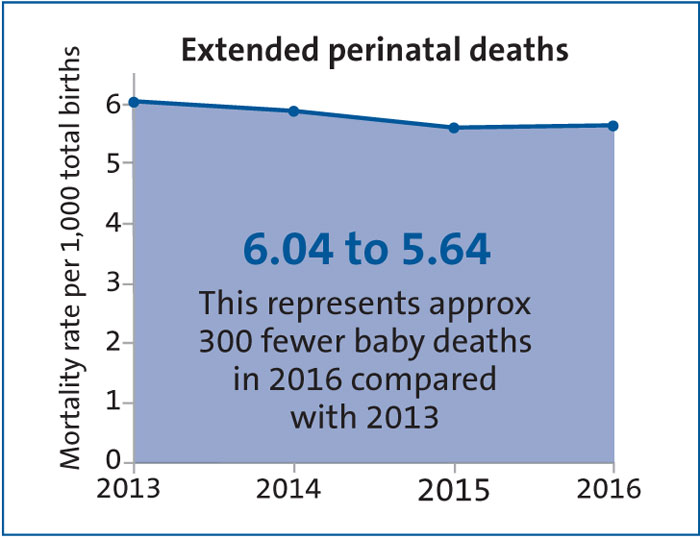
FIGURE 1 Overall reduced extended perinatal mortality rates between 2013 and 2016.
In terms of the individual constituents of extended perinatal mortality, the stillbirth rate in 2016 was 3.93 per 1,000 total births, a fall of 6.4% from 4.20 per 1,000 total births in 2013, representing 200 fewer stillbirths in 2016 compared with 2013. Following analysis to account for some of the important factors that influence the rate of death (such as poverty, mother’s age, multiple birth and ethnicity), variation in stillbirth rates across the various populations of the UK has reduced with all stabilised and adjusted rates falling to within 10% of the UK average, as indicated by all the neonatal networks being coloured either yellow or orange in the traffic light system used to highlight those areas where action is needed to improve outcomes (FIGURE 2). This suggests an equitable standard of service provision across the UK. However, UK stillbirth rates still remain high compared with many similar European countries and increased efforts should be made to try and reduce stillbirth rates in line with the best of these countries.
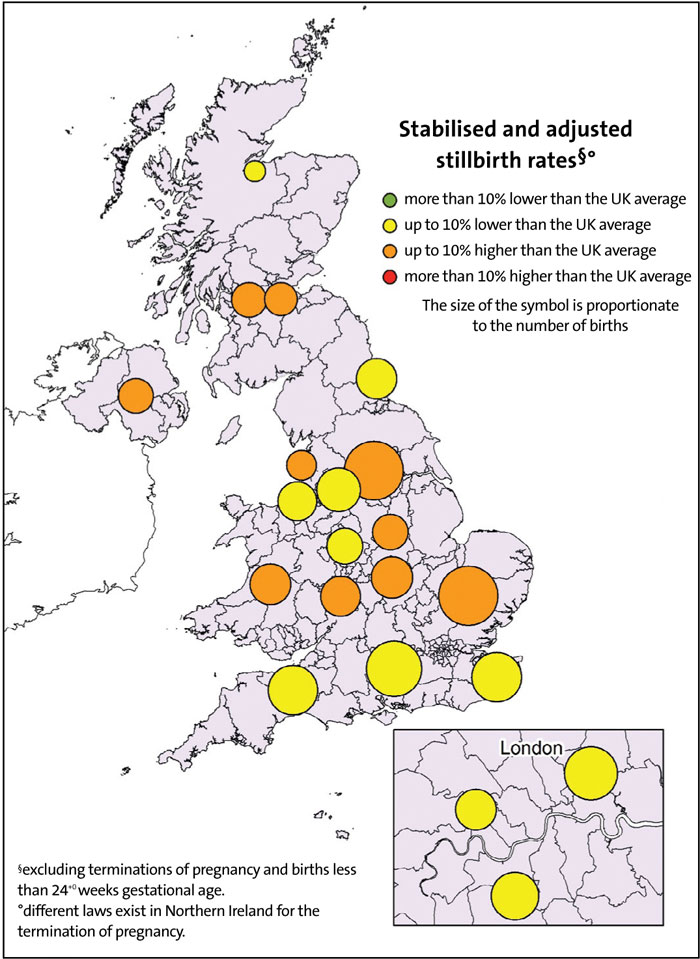
FIGURE 2 Stabilised and adjusted stillbirth rates by neonatal network based on place of birth for births in 2016.
Over the same four-year period the rate of reduction in the neonatal death rate is similar to stillbirths at 6.5%: from 1.84 to 1.72 deaths per 1,000 live births, representing 100 fewer babies dying within the first 28 days of life in 2016 compared with 2013. However, in order to achieve national ambitions to reduce these deaths more work is required to prevent these deaths in the future. There is wide variation in the stabilised and adjusted neonatal mortality rates across the various populations as shown in FIGURE 3 for the neonatal networks. Much of the variation seen in neonatal mortality rates is accounted for by differences in the proportion of babies dying from a major congenital anomaly and individual trust and health boards are provided with detailed information about all their births, stillbirths and neonatal deaths compared to the UK population as a whole to facilitate local investigation of their mortality rates.
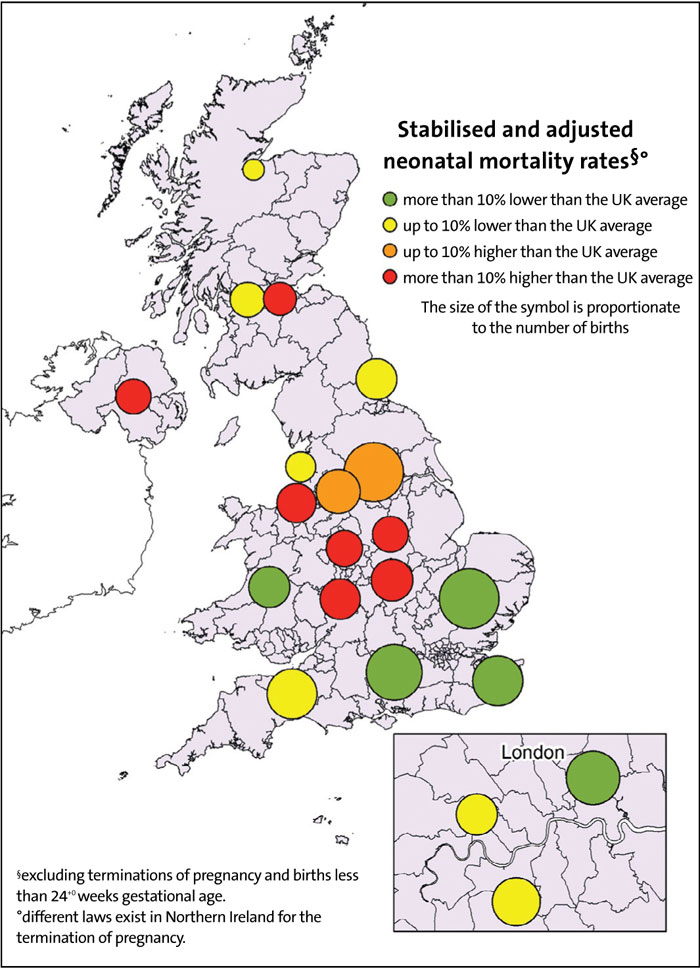
FIGURE 3 Stabilised and adjusted neonatal mortality rates by neonatal network based on place of birth for births in 2016.
Data quality and timeliness of reporting
There is a steady improvement in data quality overall, although there continues to be a problem with the completion of some maternal data especially carbon monoxide exposure monitoring (only 43.1% complete). However there is wide variation in the timeliness of reporting of deaths to MBRRACE-UK across the four countries of the UK. By the 180th day following a death, data entry has started for 95.1% cases in Wales, 86.7% in England, 71.7% in Northern Ireland and 64.0% in Scotland (FIGURE 4). In Northern Ireland data entry is carried out centrally by Northern Ireland Maternal and Child Health (NIMACH), which accounts in part for its delayed reporting. Over the past year the Perinatal Mortality Review Tool (PMRT) has been developed and launched for use across the UK to facilitate and standardise the review of all perinatal deaths within trusts and health boards. The web-based systems used for MBRRACE-UK and the PMRT are linked to allow for the sharing of data between these two programmes and to prevent the need for any duplicate data entry. In order to maximise the efficiency of this shared data the PMRT is reliant on timely data entry onto the MBRRACE-UK system and all trusts and health boards are being encouraged to start entering data onto the system as soon as possible following a death to facilitate this process. To monitor the process MBRRACE-UK is proposing two benchmarks that will be monitored in future reports:
- all deaths should be reported within 30 days
- data entry should be complete by 90 days.
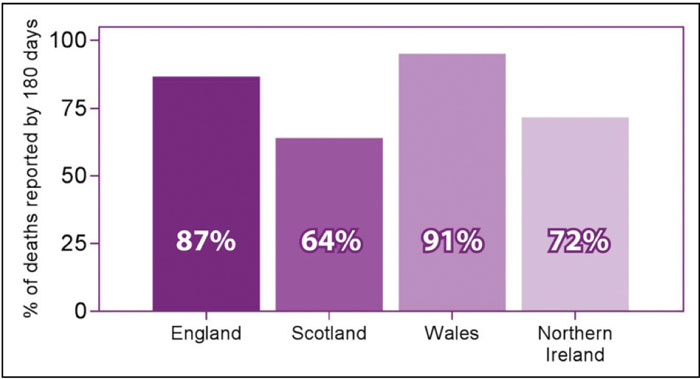
FIGURE 4 Proportion of perinatal deaths notified to MBRRACE-UK by 180 days by UK country in 2016.
Improved survival for twins
One really positive result from the latest report is that rates of both stillbirth and neonatal death associated with twin pregnancy have reduced by around one third over the period 2013 to 2016 (FIGURE 5). Over this period the increased risk of stillbirth and neonatal death in twin pregnancies compared to singleton pregnancies has also reduced by just less than a third. Multiple births have been a relatively neglected area of research in terms of reducing perinatal mortality rates. In our upcoming MBRRACE-UK confidential enquiry we are addressing this issue and carrying out an enquiry into the care provided for a random sample of twin pregnancies that resulted in the loss of at least one baby as a late fetal loss, stillbirth or neonatal death. We have held a Topic Expert Group to establish the enquiry and are currently finalising the study materials. If you have a particular interest in multiple births and would like to be an MBRRACE-UK review panel member, please contact MBBRACE-UK (tel: 0116 2525425 or email: mbrracele@npeu.ac.uk).
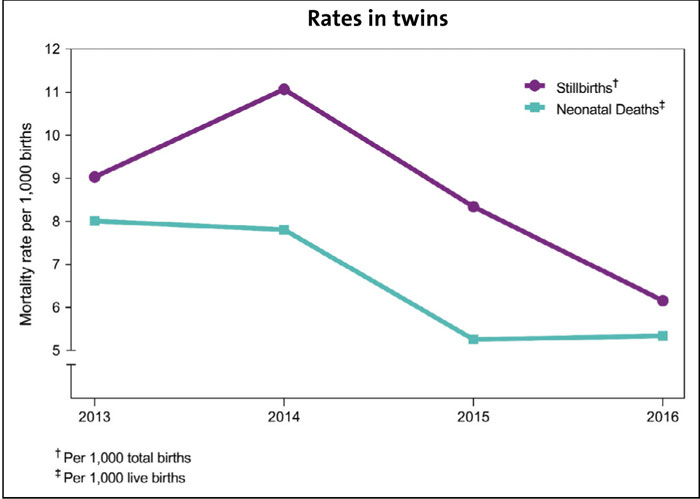
FIGURE 5 Stillbirth and neonatal death rates for twin pregnancies in the UK, 2013-2016.
The main report contains full details of all the key findings from the 2016 data. On behalf of MBRRACE-UK we would like to thank all of the reporters in the trusts and health boards across the UK. Without your support and dedication we would be unable to produce our reports and identify key issues and factors that may help in reducing UK stillbirth and neonatal death rates.
MBRRACE-UK is one of the clinical outcome review programmes funded by the Healthcare Quality Improvement Partnership. Please follow us on Twitter @MBRRACE-UK or visit our website: www.npeu.ox.ac.uk/mbbrace-uk.
Or read this article in our
Tablet/iPad edition
